VA Rating for Gout: What Veterans Should Know
Gout is one of the most frequently misunderstood conditions in the VA disability system. Many veterans experience significant daily impairment from acute flare-ups and chronic joint damage yet receive ratings that do not reflect that clinical reality. The disconnect is rarely about the severity of the condition itself—it is almost always about the evidence presented and how well it aligns with the specific criteria the VA applies.
This guide breaks down the regulatory framework that governs a VA rating for gout, explains how the VA evaluates this condition and the medical and evidentiary factors considered in that process., and identifies the medical and evidentiary factors that determine how the VA evaluates this condition. Understanding these elements is the foundation of an accurate disability evaluation.
TL;DR
- Diagnosis is the prerequisite: Elevated uric acid levels alone are insufficient. The VA requires documented evidence of uric acid crystals, clinical observation of flare-up characteristics, or imaging confirming joint involvement.
- Secondary claims are a common pathway: Many veterans successfully connect gout to a service-connected condition such as hypertension or PTSD, rather than establishing a direct in-service origin.
- Frequency drives the rating: Ratings of 20%, 40%, and 60% are determined primarily by the number of provider-documented “incapacitating episodes” per year.
- Joint damage is an alternative basis: Veterans without frequent flare-ups may still qualify for a rating based on permanent joint stiffness or limitation of motion caused by chronic gout.
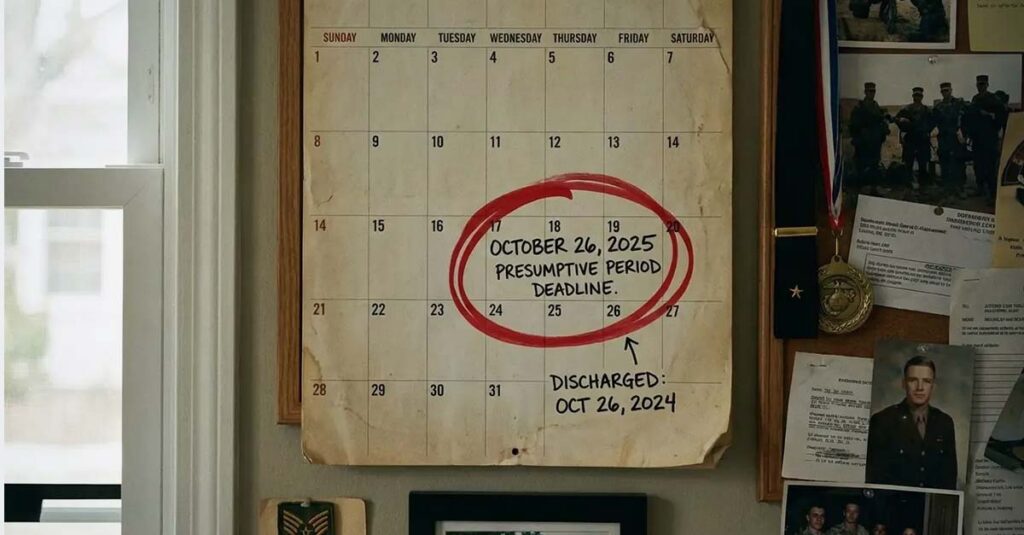
- The one-year presumptive rule: Per 38 CFR 3.309(a), gout that manifests to a compensable degree within one year of separation from active duty is presumed service-connected.
- Documentation determines outcomes: A complete independent medical opinion and a thoroughly completed DBQ are the most consequential evidentiary components in a gout va disability rating evaluation.
Proving Gout Is Service-Connected
Establishing service connection is the threshold requirement for any VA disability compensation. Without a documented link between the condition and military service, a diagnosis—regardless of severity—does not produce a rating. This is the stage at which many VA disability for gout claims are denied, and it is where evidentiary preparation is most critical.
The Basics of a Gout Claim
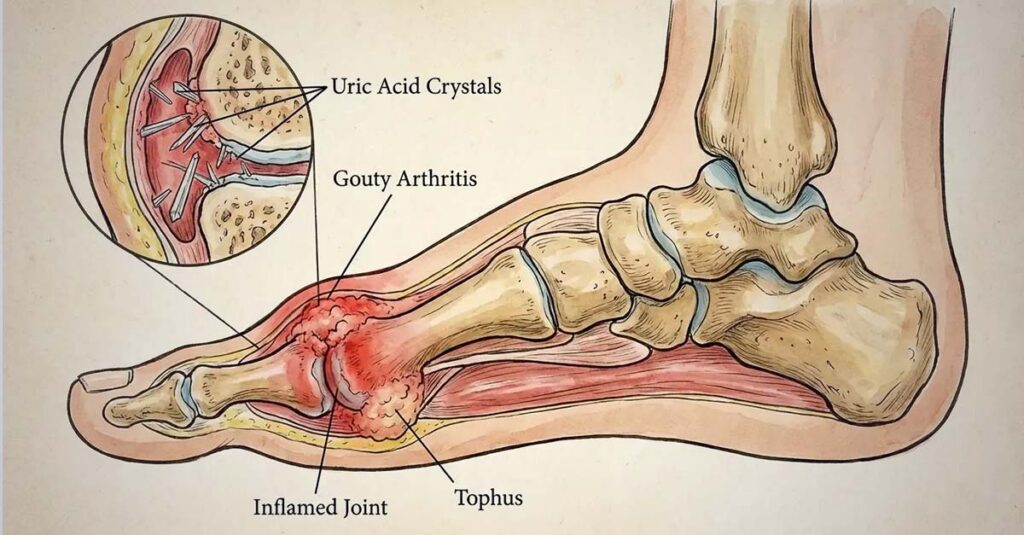
Is gout a disability under VA regulations? The answer is yes—but with conditions. The VA distinguishes between a laboratory finding and a compensable medical condition. Hyperuricemia—elevated uric acid in the blood—is a metabolic marker, not a compensable disability on its own. A compensable gout claim requires documented clinical manifestations: acute joint inflammation, confirmed crystal deposition, or radiographic evidence of joint involvement. The lab result alone does not satisfy this standard.
What the VA Needs to Diagnose Gout
The VA requires a current medical diagnosis of gouty arthritis supported by objective clinical evidence. Subjective symptom reports, absent supporting documentation, are not sufficient for rating purposes. What evidence is needed for a disability claim clarifies the specific documentation standards applicable across disability types, including the imaging and laboratory records relevant to metabolic joint conditions.
Essential Diagnostic Evidence Checklist:
- Lab results: Blood test documenting elevated uric acid levels (hyperuricemia)
- Synovial fluid analysis: Presence of monosodium urate crystals (the clinical gold standard for diagnosis)
- Imaging: X-rays showing joint damage or “rat bite” erosions; dual-energy CT (DECT) scans where applicable
- Clinical notes: Physician documentation of redness, heat, swelling, and acute tenderness in a specific joint

Direct Service Connection
Direct service connection for gout requires evidence that the condition originated during active duty. Because gout is a metabolic condition that frequently develops or worsens in middle age, direct connection is often the most challenging pathway. Service treatment records must reflect either a formal diagnosis during service or documented clinical episodes consistent with gouty arthritis. A single notation of joint pain without accompanying laboratory confirmation or clinical characterization is generally insufficient to establish the direct link.
The Direct Connection Challenge:
A veteran served in the Navy for four years and experienced one episode of significant foot pain during a deployment. The treating corpsman documented “foot pain” and provided ibuprofen—no laboratory work was ordered and no formal diagnosis was recorded. Years later, a formal gout diagnosis is established in the civilian medical record. The VA denies service connection because the service record reflects only a nonspecific symptom, not a diagnosed condition. Bridging the gap between that in-service episode and the current diagnosis requires a lay statement from a witness who observed the acute episode and an independent medical opinion establishing that the documented event is clinically consistent with the subsequent diagnosis. The VA evaluates this type of evidence as part of its determination.
Presumptive Service Connection: The One-Year Rule
Under 38 CFR 3.309(a), gout is classified as a chronic disease eligible for presumptive service connection. A va rating for gout is presumed service-connected when the condition manifests to a compensable degree—10% or greater—within one year of separation from active duty. Veterans who experienced their first documented gout flare within this window do not need to establish a direct in-service origin. The VA presumes the connection based on the proximity to service.
Connecting Gout to Other Disabilities: Secondary Claims
Gout frequently develops as a downstream consequence of other service-connected conditions or their treatments. Secondary service connection is an established pathway for veterans whose gout did not originate directly during service but is causally related to a condition or medication that did. This is a frequently applicable route in gout disability rating evaluations.
Common Secondary Service Connection Pathways for Gout:
| Primary Service-Connected Disability | The Causal Link | Mechanism |
| Hypertension | Medication side effects | Diuretics reduce the kidneys’ ability to excrete uric acid |
| Chronic Kidney Disease | Direct organ dysfunction | Damaged kidneys cannot filter uric acid effectively, leading to systemic buildup |
| PTSD / Depression | Lifestyle and metabolic changes | Chronic stress, alcohol use, and certain psychiatric medications affect uric acid metabolism |
| Type 2 Diabetes | Insulin resistance | Elevated insulin levels inhibit renal excretion of uric acid |
High Blood Pressure Medications and Gout
The relationship between service-connected hypertension and secondary gout is well-documented in clinical literature. Thiazide diuretics—commonly prescribed for blood pressure management—impair renal uric acid clearance, producing hyperuricemia and increasing gout risk. For veterans whose hypertension is service-connected and who are prescribed diuretic therapy, a secondary gout claim may be supported by pharmaceutical evidence and an independent medical opinion establishing the causal relationship. Understanding the current VA rating for hypertension provides context for how that primary condition functions as the basis for a secondary gout evaluation.
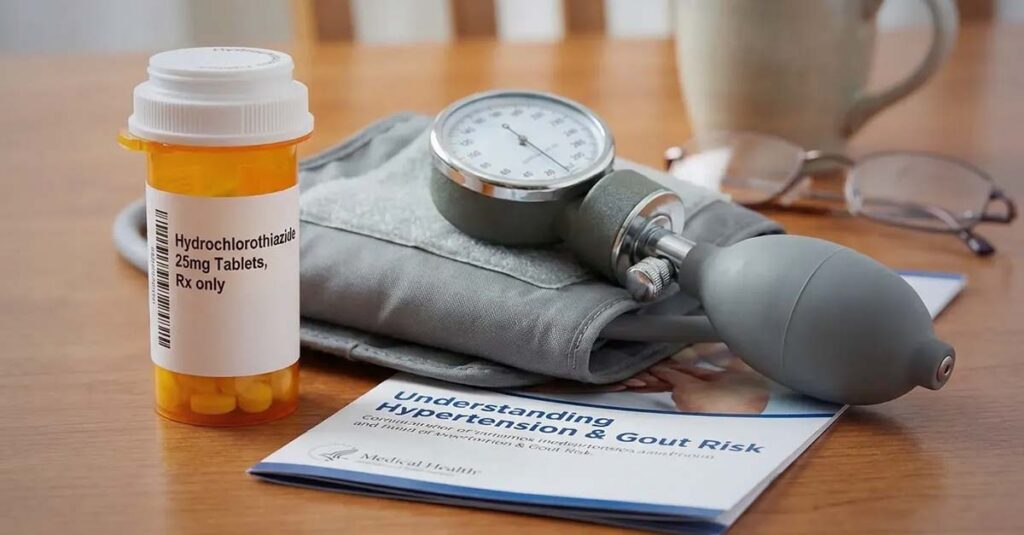
The Hypertension-Gout Connection in Practice:
A veteran rated at 10% for hypertension is prescribed hydrochlorothiazide by a VA physician. Several months later, she experiences her first acute gout flare in the knee. A secondary claim documents the chronological relationship between the diuretic prescription and the gout onset, supported by medical literature on hydrochlorothiazide-induced hyperuricemia and an independent medical opinion from a licensed physician reflecting the causal relationship. The VA evaluates this evidence as part of its secondary service connection determination.
The Connection Between PTSD and Gout
The physiological pathway between PTSD and gout operates through what is clinically described as the “intermediate step” theory. Chronic psychological stress associated with PTSD produces hormonal and metabolic changes—including elevated cortisol and insulin resistance—that impair uric acid excretion. PTSD-related behavioral patterns such as alcohol consumption and physical inactivity further increase uric acid production and retention. Additionally, certain psychiatric medications used to treat PTSD carry metabolic side effects that elevate gout risk. When filing this type of secondary claim, ensuring the primary mental health condition is thoroughly documented through the PTSD DBQ supports the evidentiary foundation of the secondary connection.

Decoding the VA Gout Rating Scale
Service connection establishes eligibility; the rating percentage determines compensation. The VA evaluates gout va disability rating determinations under two primary diagnostic codes: DC 5017 (Gout) and DC 5002 (used when gout has produced multi-joint chronic impairment). Both codes rely on objective clinical measures—not subjective pain reports—to assign a rating percentage. For a broader explanation of how these percentages combine with other service-connected conditions to determine total compensation, understanding a VA disability rating provides the relevant methodology.
Diagnostic Codes 5002 and 5017 Explained
DC 5017 applies to active gout evaluated on the basis of incapacitating episode frequency or limitation of motion. DC 5002 applies when gout has caused chronic, multi-joint impairment. The rating formula under both codes centers on two measurable clinical factors: the number of physician-prescribed incapacitating episodes within a 12-month period, and the degree of functional limitation caused by permanent joint involvement.
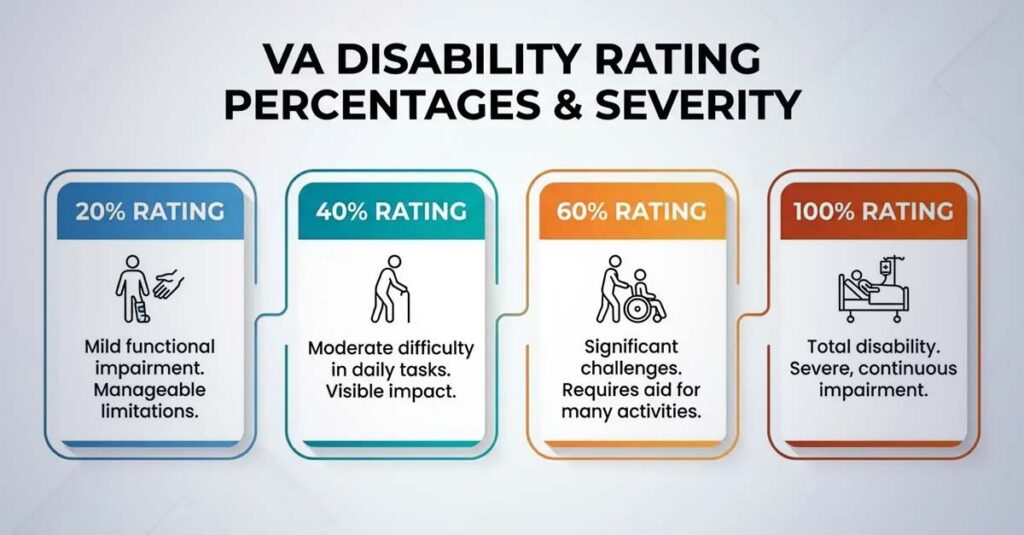
Breaking Down the Percentages
VA Rating Criteria for Gout (Diagnostic Code 5002/5017):
| Rating | Incapacitating Episodes Requirement | Alternative: Limitation of Motion |
| 20% | 1–2 incapacitating episodes per year | X-ray evidence of 2 or more major joints involved |
| 40% | 3 or more incapacitating episodes per year | Significant limitation of motion (varies by joint) |
| 60% | 4 or more incapacitating episodes per year | Weight loss, anemia, and severe functional impairment |
| 100% | Totally incapacitating; bedridden | Ankylosis (joint fusion) in an unfavorable position |
Ratings of 10% may also be assigned based on limitation of motion when incapacitating episodes are absent or infrequent but imaging confirms structural joint involvement. Reviewing how the VA calculates a VA disability rating provides additional context for how individual ratings combine into a total compensation figure.
What Counts as an “Incapacitating Episode”
The VA applies a precise clinical definition to this term in any gout va disability rating evaluation. An incapacitating episode is not defined by the veteran’s subjective experience of pain or functional difficulty. It is defined as a period during which a physician has prescribed bed rest and treatment for the condition. Flare-ups managed independently without clinical documentation do not meet this standard. Each episode must be reflected in the medical record by a treating provider who prescribed rest and treatment as part of clinical management.
Ratings Based on Limitation of Motion
When incapacitating episodes are infrequent or absent, the rating may be assigned on the basis of functional joint limitation. The VA measures range of motion using a goniometer—a clinical instrument that quantifies the degree of flexion and extension available in the affected joint. Radiographic evidence of joint degeneration, erosion, or structural damage supports this alternative rating basis. Veterans whose gout has produced permanent joint changes may qualify for a rating reflecting those structural findings even during periods of clinical remission.

Building a Complete Claim File
Diagnostic criteria and rating thresholds are objective, but they only produce accurate outcomes when the clinical record contains the specific data those criteria require. A claim built on incomplete or non-specific documentation will not produce a rating that reflects actual disability severity.
Evidence Is the Foundation
Objective documentation—laboratory records, imaging, physician observations, and medication histories—constitutes the evidentiary basis on which ratings are assigned. Gaps in this documentation produce gaps in the rating.
Medical Records and Independent Medical Opinions
Current treatment records documenting the diagnosis, flare-up frequency, and prescribed interventions form the baseline evidentiary layer. For secondary claims, an independent medical opinion documents the causal relationship between the primary service-connected condition and the gout. This opinion includes the clinical rationale supporting the conclusion that the secondary condition is at least as likely as not caused or aggravated by the primary condition. Because the causal link between conditions is not always self-evident from the record alone, understanding how a nexus letter for VA claims is structured clarifies what clinical language and documentation satisfies the VA’s evidentiary standard.
The Disability Benefits Questionnaire
The Disability Benefits Questionnaire (DBQ) is the primary document through which clinical findings are translated into the specific language and format the VA rating authority applies. A thoroughly completed DBQ that explicitly documents the number of annual flare-ups, the physician-prescribed nature of each incapacitating episode, and objective range-of-motion measurements gives the rater the precise data needed for an accurate determination. A va rating for gout claim supported by a complete DBQ substantially reduces the risk of an inaccurate rating based on documentation gaps.
DBQ Review Checklist:
- Formal diagnosis of gout confirmed
- Specific number of annual flare-ups recorded (e.g., “3 episodes in the past 12 months”)
- Range of motion documented with goniometric measurements
- Notation confirming whether flare-ups required physician-prescribed bed rest and treatment
The Filing Process
VA Form 21-526EZ is the standard form for initiating a disability compensation claim or requesting a rating increase. For secondary claims, the disability description field reflects the secondary relationship explicitly—for example, “Gout secondary to Service-Connected Hypertension.” This framing directs the VA’s review toward the relevant primary condition records and the causal evidence rather than evaluating the claim as a standalone direct service connection filing.
Framing the Claim:
When gout is evaluated as secondary to another service-connected condition, the medical documentation should clearly reflect that clinical relationship.
Understanding VA Review Options
The VA’s rating determinations are not final. When a claim is denied or a rating does not accurately reflect the clinical evidence, the VA’s decision review system provides structured pathways for re-evaluation.

Higher-Level Review
A Higher-Level Review requests that a senior VA adjudicator re-examine the existing record. No new evidence is introduced; the review assesses whether the prior determination correctly applied the rating criteria to the evidence already on file. This lane is most appropriate when the evidentiary record is complete but the rating outcome appears inconsistent with the documented clinical findings.
Supplemental Claims
According to the VA, a Supplemental Claim is the appropriate pathway when new and relevant evidence—such as an updated independent medical opinion, additional laboratory records, or a newly completed DBQ—has not yet been reviewed. This is the most direct route when a prior denial was based on insufficient documentation rather than a legal dispute about the applicable criteria.
Board of Veterans’ Appeals
When a claim involves a complex legal or medical question—such as a contested secondary service connection theory or a disputed incapacitating episode count—the Board of Veterans’ Appeals provides review by a Veterans Law Judge. This pathway involves longer processing timelines but allows for a more thorough evidentiary and legal review than the administrative lanes.
Why Independent Medical Evidence Matters
C&P examinations are conducted under significant time constraints, and the documentation produced may not capture incapacitating episode frequency, range-of-motion findings, and secondary causal relationships in the specific format the rating authority requires. When the C&P report does not fully reflect the clinical picture, the rating reflects the documentation—not the disability.
REE Medical connects veterans with independent, licensed healthcare professionals who complete DBQs and medical evaluations with the clinical thoroughness that a va rating for gout determination requires. Documentation coordinated through REE Medical is objective, VA-compliant, and prepared by providers experienced in disability-focused clinical reporting. REE Medical operates on a flat-rate model—no percentage of future benefits is taken and pricing is transparent. For veterans whose gout has not been accurately documented in terms of flare-up frequency, joint involvement, or secondary causal relationships, independent evaluation through REE Medical’s network generates the clinical record the VA can review.
Veterans can learn more about coordinating independent medical documentation by contacting REE Medical for a complimentary informational consultation.
Final Thoughts
Gout is a legitimate, compensable disability under VA regulations—but only when the clinical record reflects the specific evidentiary criteria the rating schedule requires. Flare-ups without physician-prescribed treatment do not meet the definition of incapacitating episodes. Secondary connections without independent medical opinions do not establish causation in the record.
A va rating for gout that accurately reflects disease severity depends on objective diagnosis, documented incapacitating episode frequency, and—where applicable—a clearly supported causal link to a service-connected primary condition. Veterans who understand these criteria and have medical records that reflect them are in a substantially stronger position to ensure the full clinical picture is clearly documented.
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (“VA”). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veteran’s Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.