VA Rating for TMJ: Why Jaw Pain Is Often Rated Under the Wrong Body System
Temporomandibular joint (TMJ) disorders present a documentation and classification challenge within the VA’s disability rating system. The rating criteria focus heavily on measurable jaw movement, but many veterans experience a broader range of functional limitations — chronic headaches, neck tension, sleep disruption, and dietary restrictions — that may not be fully captured during a standard examination. This disconnect between evaluation criteria and clinical reality can affect how conditions are documented and, ultimately, how they are rated. This article examines how the VA rating for TMJ works, where documentation gaps commonly occur, and what type of medical evidence may provide a more complete clinical picture.
Why the VA’s Rating Approach May Not Reflect the Full Clinical Picture
The VA evaluates TMJ disorders primarily under Diagnostic Code 9905, which falls within the dental and oral conditions category of the rating schedule. The criteria center on inter-incisal range of motion — the measurement in millimeters of how far a veteran can open their jaw between their front teeth — along with lateral excursion and the presence of structural conditions such as ankylosis. Pain, absent a direct and documented impact on range of motion, does not have an independent rating pathway under this code. Functional limitations such as dietary restrictions, headache frequency, or sleep disruption do not factor into the primary rating unless they are separately claimed and documented as distinct conditions.

Research on combat veterans reflects a well-established connection between service-related stress, trauma, and TMJ dysfunction. Studies comparing war veterans with and without PTSD to civilian populations have found that veterans with PTSD show significantly worse TMJ function and higher rates of pain during muscle palpation, with much of the dysfunction traceable to trauma sustained during service. For many veterans, TMJ is not an isolated dental condition — it is part of a broader pattern of service-connected physical impact that the primary rating code may not fully capture.
The Body System Classification Problem
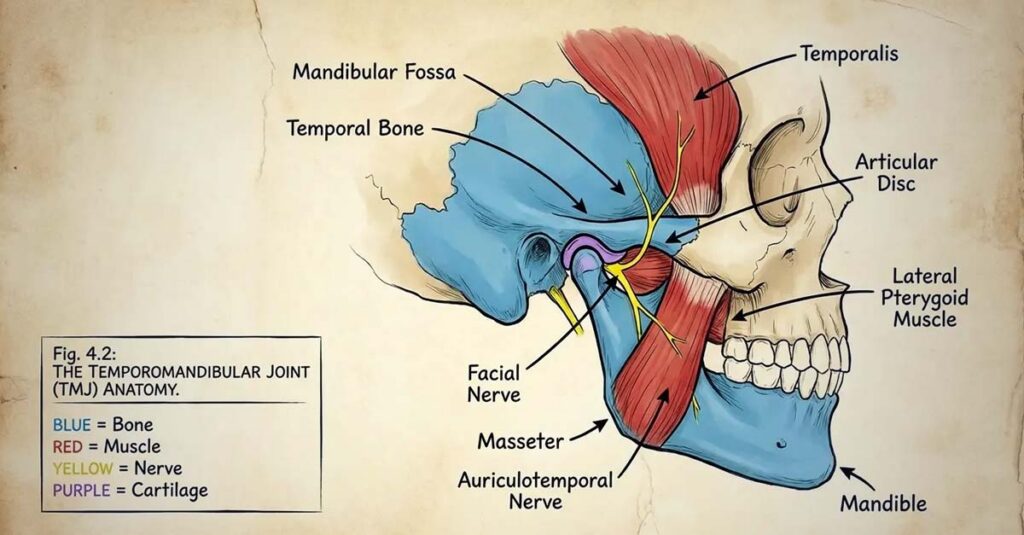
The temporomandibular joint involves interconnected muscle, ligament, disc, and bone structures, and dysfunction in this joint can produce symptoms that extend well beyond the oral cavity — including muscle tension in the face, neck, and shoulders; neurological symptoms such as facial nerve pain and referred headaches; and sleep disruption related to bruxism or clenching. A C&P examination focused on dental conditions typically evaluates jaw opening, bite alignment, and joint sounds. The myofascial pain component, neurological symptoms, and sleep-related effects fall outside the scope of that examination and, absent an explicit secondary claim with supporting medical evidence, will not be independently evaluated or rated.
Understanding VA disability ratings requires recognizing how the categorical structure of the rating schedule operates and where it may not fully reflect a condition’s clinical presentation. A veteran with documented jaw opening above the threshold for any percentage under Diagnostic Code 9905 may still experience constant muscle spasms, debilitating headaches multiple times per week, significant dietary restrictions, and disrupted sleep — none of which factor into the primary rating if they are not separately documented and claimed.
The Rating Thresholds Under Diagnostic Code 9905
The rating percentages available under Diagnostic Code 9905 are as follows:
- 10%: Inter-incisal range of 21 to 30 millimeters, or lateral excursion of 4 to 7 millimeters
- 20%: Inter-incisal range of 11 to 20 millimeters, or lateral excursion of less than 4 millimeters
- 30%: Inter-incisal range of 0 to 10 millimeters
- 40%: Ankylosis of the temporomandibular articulation with the mandible immobilized at a point that interferes with mastication and speech
The criteria are almost entirely objective and measurable. Pain is not independently rated under this code unless it directly limits motion beyond what a structural measurement would reflect. The VA’s Painful Motion principle provides that when joint movement is painful, at minimum a 10% rating may apply — but this requires that pain during movement be explicitly documented in the examination record. If the examiner does not record pain levels during range of motion testing, or does not note that pain limits functional movement beyond the structural measurement, that principle cannot be applied to the rating determination.

Lateral excursion — side-to-side jaw movement — is a required measurement under the rating criteria but is not consistently taken during all C&P examinations. Veterans with relatively preserved vertical opening but severely restricted lateral motion may have a significant functional limitation that goes unrecorded if that measurement is not performed. Measurements can also vary depending on examination conditions: pain levels, recent flare-up status, and fatigue at the time of examination can all affect recorded findings. A veteran examined during a lower-symptom period may produce a measurement that does not reflect their typical or worst-case functional limitation, which is the standard the VA rating system is intended to assess.
The Documentation Gap That Affects Rating Accuracy
C&P examinations for TMJ are frequently brief, and information that does not appear in the formal report can be as consequential as what does. Pain levels during movement are often noted but not formally recorded with sufficient specificity. Functional limitations beyond raw measurements — the inability to sustain chewing for more than a few minutes, the elimination of certain food textures from the diet, jaw locking during ordinary activities — may be mentioned conversationally but not captured in a way that influences the rating determination.
Flare-up frequency and severity are particularly difficult to document within a single examination. TMJ disorders are often episodic, with periods of relative manageability alternating with more severe episodes. If an examination occurs during a lower-symptom period and there is no supporting documentation of worse periods, the rating may reflect the better end of a variable spectrum rather than the condition’s typical functional impact.
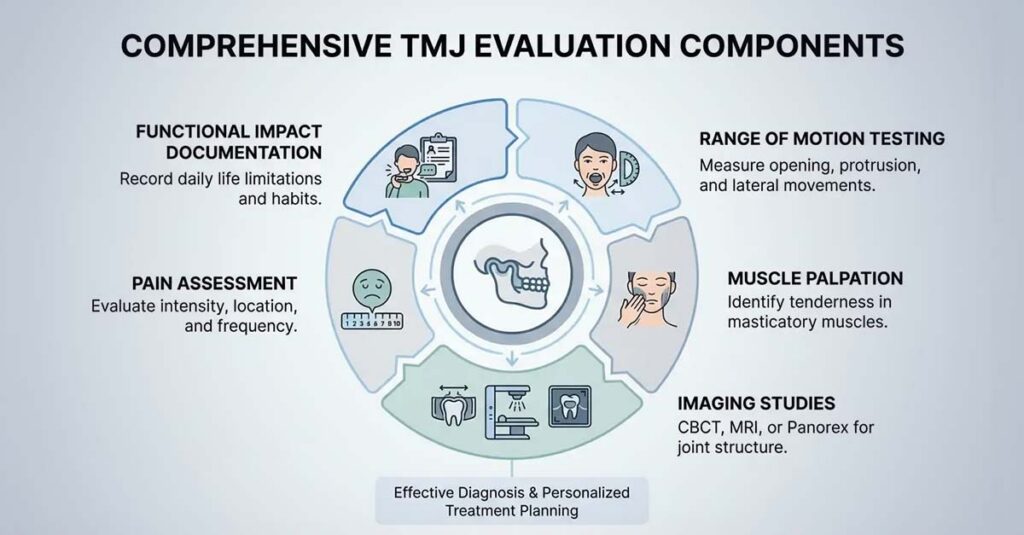
A complete TMJ evaluation relevant to disability rating should include the following:
- Inter-incisal range measurement in millimeters
- Lateral excursion measurement in millimeters
- Protrusive movement measurement
- Pain level during each range of motion measurement, recorded on a standardized scale
- Documentation of whether pain limits motion beyond structural restriction
- Characterization of joint sounds (clicking, popping, crepitus)
- Palpation findings for the joint and surrounding musculature, including the masseter, temporalis, and pterygoid muscle groups
- Assessment of occlusal alignment
- Flare-up frequency and duration
- Functional limitations including dietary modifications, chewing duration tolerance, and speech impact
- Sleep impact, including bruxism and pain-related awakening
- Any compensatory posture or behavioral changes
- Response to prior treatment
When these elements are absent from a C&P examination report, veterans have the option to request a re-examination, submit a personal statement detailing omitted functional limitations, or obtain an independent medical evaluation that addresses what the VA examination did not document. The VA is required to consider all relevant evidence submitted, regardless of its source.

Secondary Conditions: What TMJ Can Cause and Why They Require Separate Claims
TMJ disorders do not exist in clinical isolation. The muscle pathology, chronic pain, and compensatory behavioral patterns associated with the disorder can produce secondary conditions that are independently ratable — but only when they are separately claimed and supported by medical evidence establishing the causal connection to the service-connected TMJ condition.
Chronic headaches and migraines are among the most commonly associated secondary conditions. The muscles involved in TMJ disorders — particularly the masseter and temporalis — refer pain to the head and face, and trigger points in these muscles can produce tension headaches or migrainous symptoms. When headache frequency correlates with jaw pain or clenching activity and a qualified provider documents the clinical connection, migraines may be rated separately under the VA’s migraine rating criteria.
Cervical spine conditions can develop from altered head and neck posture resulting from compromised jaw function. Unconscious compensatory adjustments in head position can produce muscle imbalances and strain over time. Cervical radiculopathy or chronic cervical strain attributable to TMJ-related postural compensation may be ratable as secondary conditions with appropriate clinical documentation.
Sleep disorders are a frequently overlooked secondary condition. Bruxism and clenching during sleep are common features of TMJ disorders and can significantly disrupt sleep quality and duration. Sleep bruxism is often only detected when seeking treatment for symptoms such as headaches, facial or jaw pain, or worn-down teeth, and dental professionals note it can lead to enamel loss, tooth sensitivity, and increased cavity risk. When a veteran’s TMJ disorder is causing or materially aggravating a sleep disorder, that condition can be claimed separately with appropriate documentation.
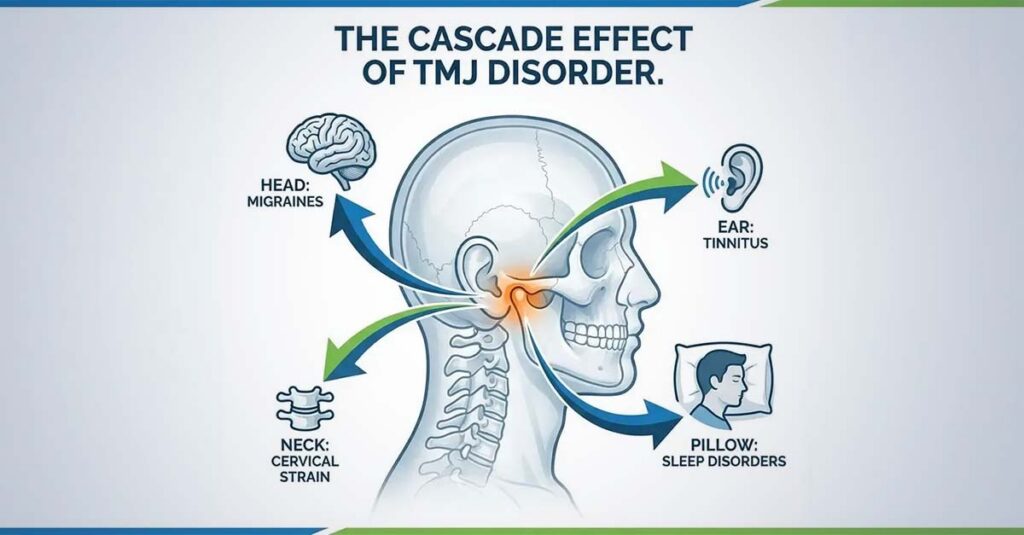
Tinnitus may be connected to TMJ dysfunction through anatomical proximity. The temporomandibular joint sits immediately adjacent to the structures of the ear, and dysfunction in the joint can affect nearby muscles and nerves. Medical literature supports this relationship: research has found that tinnitus without corresponding hearing loss may be a significant indicator of undiagnosed TMJ dysfunction, and that inflammatory processes associated with TMJ disorders may affect adjacent ear structures. A veteran who notices that tinnitus fluctuates with jaw clenching or TMJ flare-ups should have that correlation explicitly documented by a qualified provider.
Mental health conditions may be aggravated by chronic TMJ pain. The combination of persistent discomfort, sleep disruption, social avoidance, and dietary limitation associated with severe TMJ disorders may worsen existing anxiety or depressive conditions. Where a service-connected mental health condition is documented, an aggravation claim supported by clinical evidence may be appropriate.
For each secondary condition, the VA requires medical evidence — ideally a formal clinical opinion — stating that it is “at least as likely as not” that the condition was caused or materially aggravated by the service-connected TMJ disorder. Without that documentation, each condition will be evaluated independently for direct service connection, which is generally a more demanding standard to meet.
An Army veteran rated at 20% for TMJ subsequently developed severe migraines. His treating provider documented in clinical notes that the migraines appeared to originate from muscle tension in the jaw and temples and correlated with TMJ flare-up periods. He filed a secondary claim supported by a nexus opinion from a neurologist attributing the migraines to TMJ-related muscle dysfunction at the “at least as likely as not” standard, along with a headache diary documenting approximately two prostrating episodes per month. The secondary claim was approved, producing a combined rating substantially higher than the primary TMJ rating alone. The outcome depended on recognizing that migraines constituted a separately ratable condition requiring independent documentation and a dedicated claim — not a symptom to be noted in passing during a TMJ examination.

Documenting Functional Limitations Associated with TMJ
A well-supported TMJ claim is built on consistent and specific medical documentation. Regular treatment with a dentist, oral surgeon, or TMJ specialist generates a longitudinal record of symptoms, clinical observations, treatment attempts, and outcomes. Providers should be asked to document functional limitations with specificity — not merely that pain is present, but what activities are affected, what dietary modifications have been required, and how symptoms have changed over time.
A personal statement from the veteran provides context that clinical records alone may not capture. Effective personal statements describe concrete functional impacts: the specific food textures eliminated from the diet, the duration of chewing tolerance before fatigue or pain onset, the frequency with which activities involving meals are avoided, the experience of jaw locking during ordinary activities, and the effect of flare-ups on work performance. Specific and measurable descriptions carry more weight in the rating process than general statements about discomfort.
Lay statements from spouses, family members, or close observers can supplement the record by documenting observed behaviors — teeth grinding during sleep, jaw pain upon waking, dietary changes, and behavioral adaptations that reflect the condition’s ongoing functional impact. These statements provide a perspective the medical record cannot offer and can help establish the consistency and severity of symptoms across time.
Treatment compliance creates a record that reflects the persistence of the condition and its response to management. When prescribed treatments such as night guards, physical therapy, or anti-inflammatory medications are followed and documented, the record reflects both the effort to manage the condition and, where improvement is limited, the condition’s resistance to treatment. Dental professionals note that while over-the-counter mouth guards can serve as short-term solutions during high-stress periods or while awaiting professional appointments, they are not recommended for long-term use without professional supervision. Formal treatment documentation through qualified providers carries more evidentiary weight than self-directed management alone.
The timing of a claim or request for increase should account for symptom variability. Filing or presenting for examination during an atypical low-symptom period creates a record that may not represent the disability level the rating criteria are intended to capture. When symptoms fluctuate, documentation from periods of greater severity — reflected in treatment records, personal statements, or lay statements — should be included in the evidence package.
When Independent Medical Evidence Is Appropriate
Standard C&P examinations do not always provide the depth of evaluation that complex TMJ cases require. When a C&P examination is inadequate — when measurements are missing, when pain during movement is not formally recorded, or when functional limitations are not addressed in the report — veterans have the option to obtain independent medical evaluations and submit them as supporting evidence.
A thorough independent TMJ evaluation should include all relevant range of motion measurements with accompanying pain documentation, palpation findings for the joint and surrounding musculature, imaging review or referral where appropriate, and a clear functional impact assessment that addresses the specific criteria used in rating TMJ disorders. Where secondary conditions are present, the evaluation or an accompanying clinical opinion should address the causal relationship between the TMJ disorder and those conditions.
Imaging studies — including X-ray, MRI, or CT of the temporomandibular joint — can provide objective evidence of structural abnormality, disc displacement, or degenerative change that supplements physical examination findings and further supports the severity documented in clinical assessments.
REE Medical coordinates access to independent, licensed healthcare professionals who complete DBQs and medical evaluations in accordance with VA formatting and documentation standards. Providers in REE Medical’s network are experienced in disability-focused documentation, with the objective of ensuring that a veteran’s medical evidence accurately reflects the full scope of their condition — including range of motion findings, pain during movement, functional limitations, and secondary condition connections. REE Medical’s flat-rate pricing structure means veterans can access independent evaluations without variable costs, and an informational consultation is available for veterans who want to understand how independent medical documentation is coordinated and what role it plays in the VA’s evaluation process.
Final Considerations
The VA rating for TMJ is governed by criteria that prioritize measurable jaw movement over the broader clinical picture that many veterans with this condition present. The gap between a recorded rating percentage and a veteran’s actual functional experience frequently reflects what was and was not documented during the evaluation process — not necessarily the full severity of the disorder.
Understanding how Diagnostic Code 9905 operates, which secondary conditions TMJ disorders may produce and how to claim them properly, and what a complete TMJ evaluation should include provides the foundation for a more comprehensive and accurate claim. Documentation is the mechanism through which the VA’s rating system connects to clinical reality, and strengthening that documentation — through thorough independent evaluations, specific personal statements, and properly supported secondary claims — is the most direct path toward an accurate rating outcome.
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (“VA”). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veteran’s Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.