

VA Rating for Shoulder Pain: What Veterans Should Know
Shoulder conditions are among the most prevalent service-connected disabilities in the veteran population, yet according to VA Claims Insider, many Veterans may find their condition is evaluated based on specific measurement criteria.. The reason is rarely the severity of the injury itself—it is the failure to accurately apply the functional measurements the VA uses to assign compensation percentages. The rating system for shoulder conditions operates on measurable joint angles, specific legal provisions governing pain, and a framework that extends well beyond the primary diagnosis.
This guide breaks down the specific mechanics governing a VA rating for shoulder pain—from range of motion thresholds and the mandatory use of goniometric measurement, to the secondary conditions that frequently accompany shoulder injuries and the medical evidence and documentation that help provide a complete clinical picture.. For those new to the system, grasping the basics of understanding VA disability ratings is an important foundation before examining the specific joint measurements that govern shoulder claims.
TL;DR
- Range of motion drives the rating: Compensation is determined primarily by how far the arm can move, not by the diagnosis or MRI findings
- Goniometric measurement is required: If the examiner estimates joint angles without using a goniometer, the examination does not meet the required standard
- Pain during motion requires a minimum rating: Under 38 CFR 4.59, pain present during motion requires the VA to assign a minimum compensable rating, even with preserved range of motion
- Secondary conditions expand the rating: Shoulder injuries frequently produce cervical strain, radiculopathy, contralateral arm injury, and secondary mental health conditions—each potentially ratable separately
- Range of motion findings are based on when pain and limitation occur during movement.
- Repetitive use must be tested: Per De Luca v. Brown, the examiner must assess how range of motion changes with repeated use, and the post-repetition measurement is the clinically relevant metric
It Is About the Movement, Not the Diagnosis
Veterans frequently assume that a severe diagnosis—bursitis, tendonitis, or a full-thickness rotator cuff tear—automatically produces a proportionally high rating. The VA’s evaluation framework does not operate on diagnostic labels. It operates on functional impairment. The degree to which the shoulder can move, and the pain produced during that movement, is the baseline for compensation. It is important to recognize that what determines a VA rating is rarely the name of the injury but the severity of the functional limitations it causes.

Why Goniometric Measurement Is the Central Tool
A limitation of arm motion VA rating is determined through objective angular measurement of the joint, not subjective clinical impression. The instrument required for this measurement is a goniometer—a calibrated protractor designed to quantify joint angles. When a C&P examiner estimates range of motion visually rather than measuring it with this tool, the resulting angular values are clinically unreliable and do not meet the standard the VA’s own examination protocols require. An examination conducted without a goniometer produces a record that may not accurately reflect the veteran’s functional limitation.
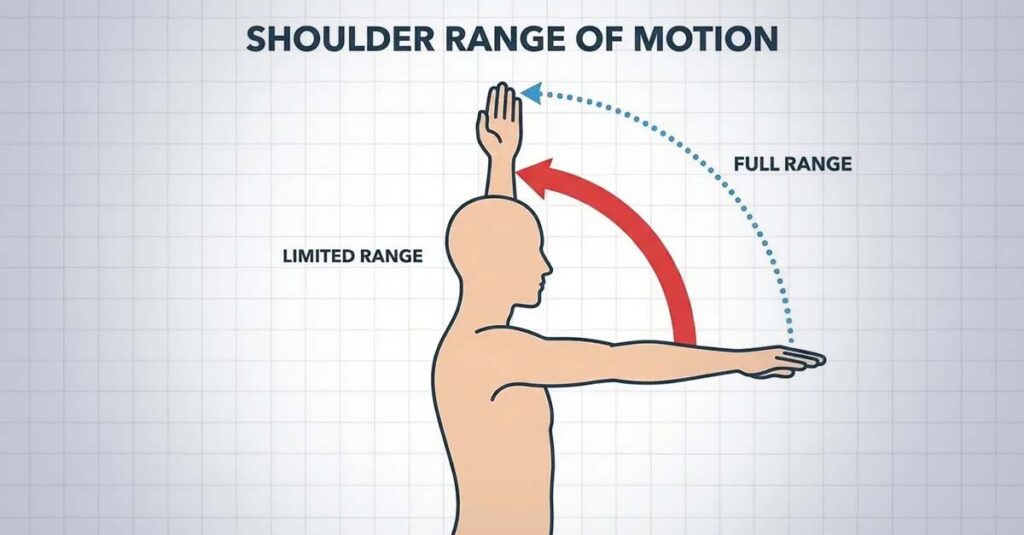
Flexion and Abduction: The Primary Measurements
The two movements most heavily weighted in shoulder evaluations are flexion—raising the arm forward—and abduction—raising the arm laterally away from the body. A healthy shoulder achieves 180 degrees in both planes. The rating thresholds under Diagnostic Code 5201 reflect decreasing functional capacity as these angles decline.
VA Rating Criteria for Limitation of Arm Motion (DC 5201):
| Arm Movement (Flexion/Abduction) | Major Arm Rating | Minor Arm Rating | Diagnostic Code |
| To 25 degrees from side | 40% | 30% | 5201 |
| Midway between side and shoulder level | 30% | 20% | 5201 |
| To shoulder level (90 degrees) | 20% | 20% | 5201 |
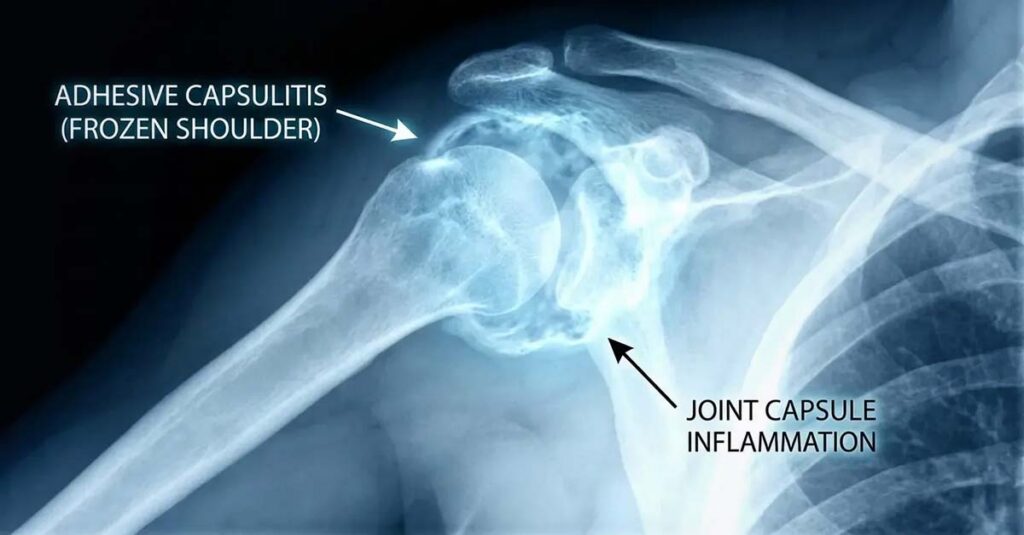
Frozen Shoulder: Ankylosis
Ankylosis—complete immobility of the shoulder joint—represents the most severe limitation category and produces the highest rating outcomes under the motion-based framework. A joint that cannot move in any plane meets the clinical definition of ankylosis. This is a high evidentiary threshold requiring documentation of total immobility, but when established, it supports ratings of up to 50% for the dominant arm.
The Painful Motion Rule: 38 CFR 4.59
The most consequential—and most frequently overlooked—provision in shoulder disability evaluations is 38 CFR 4.59. This regulation mandates that when pain is present during joint motion, the VA must assign a minimum compensable rating, regardless of whether the full range of motion is preserved. As noted by Hill & Ponton, even with full range of motion, painful motion can qualify for a minimum rating under 38 CFR 4.59, ensuring that functional impairment from pain is recognized even when mechanics appear normal.
For veterans asking what is the VA disability rating for shoulder pain when full range of motion is retained, 38 CFR 4.59 is the applicable regulatory provision. The goniometer reading does not eliminate the claim when pain is documented during the movement arc. Pain during motion must be explicitly recorded in the C&P report or DBQ to activate this protection—a veteran whose examiner does not document pain during movement loses this regulatory safeguard.
Functional Loss Beyond the Single Examination
A single C&P examination does not capture the functional reality of a chronic shoulder condition. The VA is required under 38 CFR 4.40 and 4.45 to consider functional loss—the degree of disability present during flare-up episodes, after sustained use, or at the end of a demanding workday—when assigning a rating. A measurement taken at the start of a clinical appointment, when the joint is rested, may not reflect the functional limitation experienced during occupational or daily activities.

The De Luca Factor: Repetitive Use Testing
Per the precedent established in De Luca v. Brown, VA examiners are required to assess how range of motion changes following repetitive use of the joint. If abduction measures 170 degrees on the initial attempt but decreases to 80 degrees after three repetitions due to pain, weakness, or fatigue, the post-repetition measurement is the clinically relevant metric for rating purposes.
A veteran presented at his C&P examination and raised his arm to 170 degrees on the first attempt. The examiner recorded this measurement and concluded the evaluation. The veteran’s rotator cuff pathology produced pain and mechanical limitation that restricted his abduction to approximately 80 degrees after repeated use—a limitation the examination did not capture. Under correct application of De Luca, the post-repetition functional measurement reflects the true degree of limitation, and the VA’s rating determination should be based on that functional endpoint.
Rotator Cuff, Dislocation, and Diagnostic Code Pathways
While DC 5201 governs limitation of motion and functions as the primary rating vehicle for most shoulder conditions, specific pathologies interact with the rating schedule in distinct ways. Understanding these distinctions is essential for ensuring that a VA disability rating for shoulder pain accurately reflects the applicable diagnostic framework.
Rotator Cuff Ratings
A rotator cuff VA rating is not assigned under a specific “rotator cuff tear” diagnostic code. The functional outcome of the tear—reduced range of motion, pain during movement, weakness—is what the rating schedule measures. This outcome is typically evaluated under DC 5201 or, depending on structural involvement, under codes addressing impairment of the clavicle or scapula.
Monitoring the progression of rotator cuff conditions is clinically and legally important. A 2023 study of patients in the VA health care system treated conservatively for rotator cuff disease found a 42% rate of disease progression, as noted by Hill & Ponton, indicating that an initial rating assigned at the time of service connection may not remain accurate as the condition advances.

Surgery and Convalescence
A veteran who undergoes surgical intervention for a service-connected shoulder condition may be entitled to a temporary 100% rating during the convalescence period. Upon recovery, the VA re-evaluates the condition based on residual limitation and pain. When a condition is inoperable, the rating focuses on chronic functional impairment, weakness, and pain—areas where lay statements and independent medical documentation are important for establishing the full disability picture.
Instability and Dislocation: Diagnostic Codes 5202 and 5203
Shoulder conditions involving dislocation, subluxation, or structural instability are evaluated under a distinct framework from limitation of motion claims. DC 5202 rates impairment of the humerus based on the frequency and severity of instability episodes and structural findings.
VA Rating Criteria for Impairment of the Humerus (DC 5202):
| Condition | Major Arm Rating | Minor Arm Rating | Diagnostic Code |
| Loss of head of humerus (flail shoulder) | 80% | 70% | 5202 |
| Nonunion (false flail joint) | 60% | 50% | 5202 |
| Frequent episodes of guarding | 30% | 20% | 5202 |
| Infrequent episodes, guarding at shoulder level | 20% | 20% | 5202 |
Guarding: Voluntary restriction of movement to prevent a painful or unstable shoulder from dislocating constitutes a ratable symptom. Guarding produces functional limitation that the VA must evaluate even when the joint is technically capable of greater movement.
Humerus Malunion: Fractures that heal with structural deformity or poor alignment produce separate rating considerations under DC 5202, distinct from motion limitation claims.

Secondary Conditions: The Ripple Effect
A VA rating for shoulder pain is rarely the complete picture of service-connected disability. The shoulder is a central component of upper extremity and cervical biomechanics, and its dysfunction produces downstream consequences that each carry independent rating potential. Identifying VA secondary conditions to shoulder pain is a critical component of a complete disability evaluation.
Cervical Spine Involvement
The trapezius and surrounding musculature bridge the shoulder girdle and the cervical spine. Altered mechanics from a service-connected shoulder condition—including compensatory posturing and asymmetric load-bearing—frequently produce or aggravate cervical strain. The kinetic chain relationship between shoulder and cervical spine is clinically well-established. As highlighted by Hill & Ponton in a 2024 review of military injury patterns, the prevalence of kinetic chain injuries among service members exposed to sustained heavy load-bearing and physical strain reflects how interconnected upper extremity and cervical spine pathology is in veteran populations. A secondary cervical strain claim, supported by an independent medical opinion establishing the biomechanical connection, reflects this documented relationship.
Cervical Radiculopathy
Joint swelling, inflammation, or structural compromise in the shoulder region may compress nerve roots or peripheral nerves traveling into the upper extremity, producing radiculopathy—a condition medically and legally distinct from the shoulder joint pathology. Sensory deficits including numbness and tingling in the fingers, or measurable reduction in grip strength, are clinical indicators of nerve involvement. Radiculopathy is rated under the peripheral nerve schedule and is evaluated separately from the shoulder rating, with ratings available for each affected extremity.

Contralateral Arm Overcompensation
Sustained reliance on the non-service-connected arm to compensate for a dysfunctional service-connected shoulder produces measurable wear and tear on the contralateral limb. The VA recognizes overcompensation injury as a basis for secondary service connection of the contralateral extremity. When both upper extremities carry service-connected ratings, the bilateral factor applies—adding an incremental value to the combined rating calculation.
A veteran with a service-connected right shoulder dislocation rated at 20% performed all significant physical tasks with his left arm over a five-year period, developing left shoulder tendonitis as a result. A secondary claim for the left shoulder, supported by a medical opinion documenting the overcompensation mechanism, produced ratings for both shoulders. The VA’s determination was based on the documented causal relationship between the primary service-connected condition and the secondary injury.
Secondary Mental Health Conditions
Chronic pain from a service-connected shoulder condition is a recognized basis for secondary psychiatric disability. Depression, anxiety, and somatic symptom disorders that develop as a direct consequence of chronic physical pain and functional limitation are ratable independently from the primary orthopedic condition. A VA rating for depression established as a secondary condition requires documentation of the temporal relationship between the onset of chronic pain and the development of psychiatric symptoms, supported by a clinical opinion establishing the causal link.
In Board of Veterans’ Appeals decision No. 1711810 (April 12, 2017), referenced by Hill & Ponton, a veteran was granted TDIU on an extraschedular basis after establishing that orthopedic conditions and resulting chronic pain rendered him unable to maintain substantially gainful employment. The case reflects that when service-connected physical conditions produce unemployability, the full range of secondary functional impacts must be documented and presented to the VA.

Building a Complete Evidence File
Essential Evidence Checklist for Shoulder Claims:
- Current diagnosis: MRI or X-ray confirming pathology (tear, arthritis, dislocation, structural deformity)
- Independent medical opinion: A clinical statement linking the current condition to service, or to an existing service-connected disability for secondary claims
- Personal statement (VA Form 21-4138): Detailed description of flare-up episodes, functional restrictions, and daily impact
- Lay statements: Written accounts from family members or fellow service members documenting observed limitations
- Private DBQ: An independently completed evaluation with goniometric range of motion measurements, repetitive use testing, and pain documentation
The Private DBQ
The Disability Benefits Questionnaire is the primary clinical document the rating authority uses to assign a shoulder disability percentage. A privately completed DBQ, prepared by an independent physician who measures range of motion accurately, conducts repetitive use testing, and documents pain behavior, provides a more complete clinical record than an examination conducted under significant time constraints. Utilizing a private DBQ for securing VA benefits helps ensure functional limitations are clearly documented in the medical record.
Accurate Documentation Through REE Medical
The completeness and accuracy of medical documentation play an important role in how shoulder conditions are evaluated. C&P examinations that do not apply goniometric measurement accurately, do not conduct repetitive use testing, or do not document pain during motion leave critical evidentiary gaps that produce ratings inconsistent with the veteran’s actual functional limitation.
REE Medical connects veterans with independent, licensed healthcare professionals experienced in completing shoulder DBQs and medical evaluations that meet VA documentation standards. Documentation coordinated through REE Medical is objective, VA-compliant, and prepared with specific attention to accurate goniometric measurement, repetitive motion assessment, pain documentation under 38 CFR 4.59, and secondary condition identification—including radiculopathy, cervical strain, and contralateral limb injury. REE Medical operates on a flat-rate model; no percentage of future benefits is taken and pricing is transparent. REE Medical has supported more than 95,000 veterans in strengthening their claims with compliant independent medical documentation.
Veterans can learn more about coordinating independent medical documentation by contacting REE Medical for a complimentary informational consultation.
Final Thoughts
Shoulder claims require precise measurements, accurate application of the painful motion rule, and systematic identification of secondary conditions. The VA rating for shoulder pain is not determined by the severity of the diagnosis—it is determined by the accuracy and completeness of the functional documentation in the claim file. Veterans who understand the role of goniometric measurement, the protections afforded by 38 CFR 4.59, the requirements of De Luca repetitive use testing, and the secondary condition pathways associated with shoulder pathology are substantially better positioned to receive compensation that reflects the actual impact of their service-connected disability.
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (“VA”). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veteran’s Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.


