

VA Rating for Knee Popping: Turn That Click into Compensation
Knee popping is one of the most frequently reported musculoskeletal complaints among veterans, yet many claims based on this symptom are denied or underrated—not because the condition is invalid, but because the noise alone does not constitute a ratable diagnosis under VA criteria. The VA rates the underlying pathology causing the sound: structural compromise of the joint, measurable limitation of motion, and documented functional loss. Understanding how those clinical realities translate into specific Diagnostic Codes and rating percentages is essential for any veteran navigating the VA knee rating framework.
To better navigate this system, it helps to start by understanding VA disability ratings and how specific symptoms translate into percentage points.
TL;DR
- Popping is not a diagnosis. The VA rates the underlying cause—typically instability or cartilage damage—not the sound itself.
- Instability carries weight. Documentation that the knee gives way (instability of station) is among the most direct routes to a compensable rating under Diagnostic Code 5257.
- Pain during motion matters. Under 38 CFR § 4.59, pain during movement establishes a minimum 10% rating regardless of range of motion.
- The DBQ supports evaluation. When the examining provider does not document functional loss, objective instability findings, and crepitus, the VA rater may have insufficient evidence to assign an accurate rating.
- C&P exam measurements are critical. Range of motion measurements reflect the point at which pain begins—not the maximum range a veteran can physically tolerate.
Decoding the “Pop” in VA Terms
The VA does not maintain a Diagnostic Code for the sound of knee popping. For a VA rating for knee popping to translate into compensation, the symptom must be characterized in medical and regulatory language that maps to an established code. Popping typically signals one of two underlying conditions: mechanical instability of the joint or internal derangement involving cartilage or ligamentous structures. A claim centered solely on auditory symptoms will not generate a compensable rating; a claim grounded in the pathology producing those symptoms may.
It’s Not Just Noise; It’s Pathology
The clinical term most commonly associated with joint noise is crepitus—a grinding or crackling sensation caused by irregular articulating surfaces, cartilage degradation, or loose bodies within the joint space. In other presentations, the sound reflects a ligament shifting or snapping as the joint moves through its range of motion. Both presentations indicate compromise of the knee’s structural integrity and may correspond to ratable conditions under the VA’s Schedule for Rating Disabilities. Identifying the precise mechanism—cartilage deterioration versus ligamentous laxity—determines which Diagnostic Code applies and, consequently, which rating criteria govern the claim.

Meniscal Tears and Locking
Frequent popping, particularly when accompanied by locking, catching, or acute pain during specific movements, often reflects a tear in the medial or lateral meniscus (also referred to in VA regulations as the semilunar cartilage). The VA rates meniscal pathology under Diagnostic Code 5258 (dislocated semilunar cartilage with characteristic symptoms) or Diagnostic Code 5259 (symptomatic removal of the semilunar cartilage). The noise is a symptom; the structural tear is the ratable condition. Imaging studies—typically MRI—and objective clinical tests such as the McMurray test provide the diagnostic evidence the VA reviews when evaluating this type of claim.
Ligament Issues and Shifting
When the popping sensation is accompanied by a feeling that the knee is shifting laterally or failing to track correctly, the underlying cause may involve laxity in the anterior cruciate ligament (ACL), medial collateral ligament (MCL), or posterior cruciate ligament (PCL). This presentation is clinically distinct from cartilage-related noise. Ligamentous laxity produces functional instability—an inability to bear weight reliably or maintain consistent joint alignment during ambulation. This distinction is significant within the VA rating framework because instability is evaluated under a separate Diagnostic Code from range of motion limitations and may yield an independent rating.
The “Instability of Station” Gold Mine
“Instability of station” is a specific regulatory concept under VA law referring to the knee’s inability to support the veteran’s body weight during standing or ambulation. It is the foundational basis for ratings assigned under Diagnostic Code 5257, which governs recurrent subluxation or lateral instability of the knee. When knee popping is accompanied by episodes of the joint giving way—even partially—the symptom crosses from a subjective complaint into a documentable functional impairment. Knowing what determines a VA rating regarding joint function is essential for understanding how instability evidence translates into percentage points.
Illustrative Example: Consider a veteran who reported knee popping during daily activities, and whose initial claim was denied on the basis of subjective symptom reporting. Upon appeal, medical records and a lay witness statement documented an incident in which the knee audibly popped and then buckled under load during a routine task, causing a fall. This documentation recharacterized the claim from one based on noise to one grounded in instability of station. The VA ultimately assigned a 20% rating under Diagnostic Code 5257. This example illustrates how detailed, event-specific documentation can clarify the record for VA evaluators.
Instability Rating Levels
Slight Instability (10%)
A 10% rating under Diagnostic Code 5257 reflects slight instability—a sensation of weakness or giving way that is perceptible to the veteran but does not significantly alter gait or cause frequent falls. The knee may feel unreliable, but it does not buckle completely during normal weight-bearing activities.
Moderate Instability (20%)
Moderate instability, rated at 20%, reflects episodes in which the knee actually gives way during ambulation or weight-bearing activities. The veteran may need to modify movement patterns or exercise caution when walking to prevent falls. This level of impairment is objectively distinguishable from the slight category and requires corroborating clinical findings.
Severe Instability (30%)
The maximum rating under Diagnostic Code 5257 is 30%, assigned when the veteran experiences persistent giving way or dislocation (subluxation) that necessitates the use of a brace and/or assistive device such as a cane for ambulation. At this level, the popping sensation is a precursor to near-complete loss of joint support.

VA Ratings for Knee Instability (Diagnostic Code 5257)
| Severity Level | Description of Symptoms | VA Rating |
| Slight | A sensation of “giving way” or weakness; lateral instability is present but does not cause frequent falls. | 10% |
| Moderate | Recurrent subluxation or lateral instability; the knee actually gives out occasionally; requires caution when walking. | 20% |
| Severe | Persistent giving way or dislocation (subluxation); requires the use of a brace and/or cane for ambulation. | 30% |
Mastering the VA Knee Rating Chart
The VA knee rating chart is complex because a single knee may be evaluated along three independent dimensions: limitation of motion, instability, and pain. Under the principle of evaluating the disability in its entirety, it is possible for a veteran to receive separate ratings for different functional impairments affecting the same joint—provided each rating reflects a distinct aspect of disability. Because the criteria are strict, knowing exactly what determines a VA rating regarding joint function is essential for understanding how each dimension of impairment is evaluated.
Range of Motion Rules
The majority of knee ratings are assigned based on measurable limitations in flexion (bending) or extension (straightening), expressed in degrees and evaluated against specific thresholds established in the VA rating schedule. Objective measurement using a goniometer is the standard; estimates or visual approximations do not satisfy VA evidentiary requirements.

Flexion Limitations (Code 5260)
Limitation of knee flexion is rated under Diagnostic Code 5260. A compensable rating under this code generally requires flexion limited to 45 degrees or less. Flexion limited to 60 degrees is assigned a non-compensable 0% rating. The thresholds are strict, and precise goniometric measurement is essential to establishing the documented limitation.
Extension Limitations (Code 5261)
Limitation of knee extension is rated under Diagnostic Code 5261 and reflects the veteran’s inability to fully straighten the leg. Extension limited by 5 degrees or less does not generate a compensable rating. A limitation of 10 degrees or more corresponds to a 10% rating, with progressively higher ratings assigned as the degree of limitation increases, up to 50% for extension limited by 45 degrees.
Range of Motion (ROM) Rating Criteria
| Limitation Type | Degree of Limitation | VA Rating |
| Flexion (Bending) | Limited to 60° | 0% |
| Limited to 45° | 10% | |
| Limited to 30° | 20% | |
| Limited to 15° | 30% | |
| Extension (Straightening) | Limited by 5° | 0% |
| Limited by 10° | 10% | |
| Limited by 15° | 20% | |
| Limited by 20° | 30% | |
| Limited by 45° | 50% |
The Safety Net of Painful Motion
Veterans whose range of motion falls within normal parameters but who experience pain during movement retain a protected pathway to compensation under federal regulations. This provision serves as a critical safeguard for veterans whose functional impairment is real but not fully captured by degree-based measurement alone.
The 10% Minimum Rule
Under 38 CFR § 4.59, pain during motion—including pain that accompanies or is triggered by joint noise—entitles a veteran to a minimum 10% rating for the affected joint. This standard applies regardless of how far the joint can be moved, provided that pain is documented as occurring during the range of motion evaluation. The regulatory basis for this provision reflects the VA’s recognition that functional impairment is not always measured in degrees.
Arthritis and Bone-on-Bone
When knee popping is caused by cartilage loss resulting in bone-on-bone contact, the applicable rating pathway shifts to degenerative joint disease under the arthritis codes. This change carries different evidentiary requirements from those governing instability or range of motion claims.
X-Ray Requirements
Diagnostic Code 5003 governs degenerative arthritis and requires objective radiographic evidence to substantiate the diagnosis. X-ray imaging must demonstrate the presence of osteophytes (bone spurs) or joint space narrowing. Symptom reports alone, without supporting imaging, are insufficient to establish a ratable arthritic condition under this code.

Incapacitating Episodes
Ratings for arthritis-related knee conditions can reach 20% when the veteran experiences occasional incapacitating episodes—defined as periods of acute symptom exacerbation severe enough to require bed rest or physician-directed treatment. Documentation of these episodes, including dates, duration, and treatment received, supports this rating level.
Crepitus as Objective Evidence
Crepitus documented by an examining physician during a clinical evaluation carries evidentiary weight that self-reported popping does not. When a licensed provider notes crepitus during range of motion testing—particularly in the context of an arthritic knee with accompanying pain and stiffness—that observation transforms a subjective complaint into an objective clinical finding. In the VA’s evaluative framework, objectively noted crepitus supports the application of 38 CFR § 4.59’s painful motion provision and can contribute to establishing the presence of degenerative joint changes under Code 5003.
The DBQ for Knee Pain Is Your Blueprint
The DBQ for securing VA benefits (Disability Benefits Questionnaire) is the structured medical form completed by a licensed healthcare provider to document a veteran’s condition for VA review purposes. Within the context of a knee claim, the DBQ for knee pain is among the most consequential documents in the claim file. When the examining provider does not document instability findings, crepitus, functional loss, or painful motion, the VA rater is left without the clinical basis necessary to assign an accurate rating. A properly and thoroughly completed DBQ acts as a roadmap for the rater, directing analysis to the appropriate Diagnostic Code and rating criteria.
Critical DBQ Sections
The accuracy of the DBQ depends on the completeness with which the examining provider addresses each functional domain. Each section serves a distinct evaluative purpose within the VA’s rating framework.
Documenting Functional Loss
The functional loss section of the DBQ asks whether the knee condition affects the veteran’s ability to perform occupational or daily life activities. When knee popping contributes to functional impairment—such as difficulty climbing stairs due to locking, or an inability to sustain prolonged walking due to pain and instability—those specific limitations warrant documentation. Detailed, activity-specific descriptions in this section allow the VA to evaluate disability beyond what degree measurements alone convey.
Pre-DBQ Symptom Reference List
The following are examples of the types of observations the VA may review when evaluating knee-related functional loss:
- Whether popping occurs during specific movements (e.g., squatting, climbing)
- Whether the popping causes an immediate interruption of activity
- Whether swelling or stiffness follows the popping sound
- Whether falls or stumbling have occurred due to instability
- Whether a brace, cane, or knee sleeve is used to maintain stability
Capturing Flare-Ups
The DBQ includes a section for documenting symptom severity during flare-up episodes. When knee popping and associated pain increase in frequency or intensity following physical exertion or environmental changes, this pattern carries clinical relevance. Documentation of flare-up characteristics—including triggers, duration, and symptom severity during exacerbation—provides the VA with a more complete picture of the condition’s impact over time.
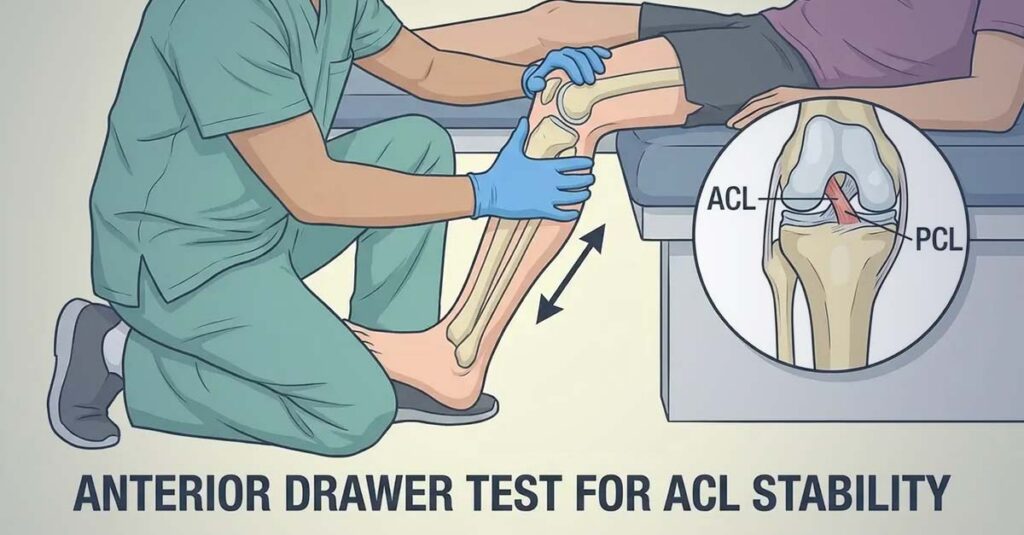
Objective Testing: Drawer and McMurray
Clinical validation of instability and meniscal pathology requires the use of objective physical examination maneuvers. The anterior and posterior drawer tests assess ligamentous integrity by evaluating the degree of anterior-posterior tibial translation. The McMurray test evaluates meniscal integrity through a specific range of motion maneuver that elicits a click or pop when a meniscal tear is present. Positive findings on either test provide objective clinical support for the veteran’s symptom reports and should be documented explicitly in the DBQ.
Precision in ROM Testing
Range of motion measurements recorded in the DBQ must be obtained using a goniometer—a calibrated angle-measurement instrument—rather than visual estimation. Imprecise measurements are not clinically or regulatorily valid for VA rating purposes. The DBQ also contains a dedicated field for documenting whether pain was present during range of motion testing; this field directly supports the application of 38 CFR § 4.59’s minimum rating provision.
Filing a Knee Claim: What the VA Reviews
Establishing a compensable VA rating for knee popping requires a claim file that objectively demonstrates the mechanical failure of the joint—through medical records, lay evidence, and clinical documentation—rather than subjective symptom reports alone. Recognizing the importance of medical evidence in VA disability claims is often the deciding factor between a denial and a favorable rating decision.
Building the Evidence File
A well-supported knee claim rests on a documented history that establishes both the chronicity of the condition and its connection to military service. Service treatment records reflecting complaints of knee pain, injuries, or diagnostic evaluations during active duty form the foundation of this history.
The Role of Lay Evidence (Buddy Statements)
Lay witness statements—submitted via VA Form 21-4138—from spouses, family members, or fellow service members can document observable manifestations of knee instability that medical records may not capture. A statement describing witnessed episodes of buckling, falls, or altered gait attributable to the knee provides the VA rater with corroborating evidence of instability that extends beyond clinical settings.
Example of an Effective Lay Statement: “I served with Sgt. Miller in the infantry. During our rucks in 2018, I regularly heard his right knee make a loud cracking sound. On two separate occasions during PT, I observed his knee buckle underneath him, forcing him to stop and sit out. He continues to walk with that same altered gait today.”
Reviewing Service Treatment Records
Service treatment records may contain documented complaints, diagnoses, or treatment related to the knee—including sprains, strains, evaluations for joint noise, or orthopedic referrals. Each relevant entry contributes to the evidentiary chain connecting the current condition to active duty service.
The C&P Examination
The Compensation and Pension (C&P) examination is the VA’s primary mechanism for evaluating the current severity of a claimed condition. According to the VA, this examination is used to assess the veteran’s diagnosis, functional limitations, and symptom severity, which the VA then uses to assign an appropriate rating.
Measurement Standards: Per VA guidance, range of motion assessments conducted during C&P examinations should use a goniometer to produce accurate degree measurements. If this instrument is not used, the examination may not meet VA standards for a sufficient examination.
Pain Documentation: The VA’s rating criteria, including the painful motion provision under 38 CFR § 4.59, depend on accurate documentation of when pain occurs during range of motion testing. Per VA policy, range of motion ratings are based on the onset of pain, not maximum range. Accurate communication of pain onset during the examination allows the examiner to record the measurement at the clinically relevant point.
Illustrative Example: If pain begins when the knee is bent to 45 degrees but is not communicated until the joint has been moved to 90 degrees, the recorded measurement will likely reflect 90 degrees—a non-compensable finding. When pain onset at 45 degrees is communicated to the examiner at that point, the documented limitation may support a 10% or higher rating under Diagnostic Code 5260. This example illustrates how the timing of pain communication during the examination affects the accuracy of the recorded measurement.
C&P Examination Reference Points
The following information reflects general VA examination practices that veterans may find useful to be aware of:
- According to VA policy, pain medication taken immediately before an examination may affect the accuracy of symptom representation during assessment.
- Loose clothing (such as shorts) allows direct access to the knee during physical examination maneuvers.
- Per VA policy, a spouse or accompanying individual may be present during the examination as an observer.
- The VA’s goniometric measurement standard applies to all range of motion assessments conducted during C&P examinations.

Responding to Low Ratings
When a veteran receives a 0% rating despite documented knee popping, pain, and functional impairment, regulatory pathways exist to pursue review of that determination. Knowing how to challenge a low VA rating can provide a structured foundation for pursuing more accurate evaluation through established VA review processes.
Supplemental Claims
According to the VA, the Supplemental Claim pathway is available to veterans who can present new and relevant evidence that was not part of the original claim record. In the context of a knee rating, this may include a private medical evaluation that specifically addresses instability of station, a newly completed DBQ for knee pain that documents crepitus and functional loss with greater clinical precision, or imaging studies that were not previously submitted. New medical evidence reopens the evaluative record and provides the VA with additional clinical information on which to base a revised determination.
Independent Medical Documentation for Knee Claims
Veterans pursuing ratings for knee popping, instability, or chronic pain may find that the standard C&P examination timeline does not allow for thorough assessment of flare-up frequency, instability of station, or the nuanced functional limitations associated with joint noise and pain. Independent medical evaluations and DBQs—completed by licensed healthcare professionals outside the VA system—provide objective clinical documentation that supplements the claim file.
REE Medical coordinates access to independent, licensed medical professionals experienced in completing VA-standardized DBQs that accurately reflect the full scope of a veteran’s knee condition. These providers understand that joint noise is a clinical symptom of underlying structural compromise and document findings accordingly—whether for an initial evaluation or a request for a rating increase. Veterans can learn more about coordinating independent medical documentation by contacting REE Medical.
Final Thoughts
Knee popping is a clinically meaningful symptom that may reflect significant structural compromise of the joint, including instability, cartilage damage, degenerative arthritis, or painful motion. The VA rating for knee popping is not assigned for the noise itself, but for the underlying pathology it represents. By understanding the applicable Diagnostic Codes—5257 for instability, 5258 and 5259 for meniscal damage, 5260 and 5261 for range of motion limitations, and 5003 for degenerative arthritis—and by ensuring that clinical documentation accurately captures the full scope of functional impairment, veterans position their claims on a foundation of objective, verifiable medical evidence. Thorough documentation is the mechanism through which the VA can accurately evaluate the true impact of the condition.
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (VA). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veterans Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.


