

VA Rating for Carpal Tunnel: Why Your Wrist Pain Deserves More Than 10%
Carpal Tunnel Syndrome (CTS) is among the most common peripheral nerve conditions affecting veterans, yet a significant number of those who file receive the minimum compensable rating of 10%—even when their symptoms substantially impair daily function and employability. The disconnect between lived experience and assigned percentage is rarely a reflection of the condition’s severity. It is more often a function of how the claim is documented, which evidence is presented, and whether the correct regulatory framework is applied during evaluation.
The VA does not rate carpal tunnel as a named syndrome. Instead, it evaluates the condition through the lens of median nerve impairment under a specific Diagnostic Code, using a clinical framework that distinguishes between dominant and non-dominant hand involvement, degrees of incomplete paralysis, and functional loss. Understanding VA disability ratings and how the administration evaluates functional loss across different body systems is the essential starting point for any veteran navigating this process.
This guide examines the full scope of the VA’s evaluation framework for carpal tunnel—from Diagnostic Code 8515 and service connection pathways to rating tiers, post-surgical adjustments, and the evidentiary standards that determine whether a claim reflects the full extent of a veteran’s condition.
TL;DR
- Diagnostic Code 8515: The VA rates Carpal Tunnel Syndrome based on paralysis of the median nerve, not the syndrome’s name.
- Dominant Hand Matters: The “Major” (dominant) hand can receive a higher rating than the “Minor” hand for the same severity of symptoms.
- Objective Evidence Is Essential: Subjective pain reports are insufficient; EMG or Nerve Conduction Studies are required to establish severity.
- Surgery Changes the Rating: A temporary 100% rating may apply post-surgery, but a re-evaluation follows once recovery is complete.
- Painful Motion Rule: Even with mild nerve damage, pain during movement may establish a minimum compensable rating under 38 CFR § 4.59.
Decoding the Diagnosis: It’s More Than Just Wrist Pain
For VA purposes, a carpal tunnel claim framed around wrist pain alone is insufficient. The VA’s rating schedule evaluates the condition through the clinical lens of median nerve impairment—a distinction that shapes how evidence must be assembled and presented. Before diving into specific codes, it is helpful to have a broad grasp of understanding VA disability ratings and how the administration evaluates functional loss across different body systems.
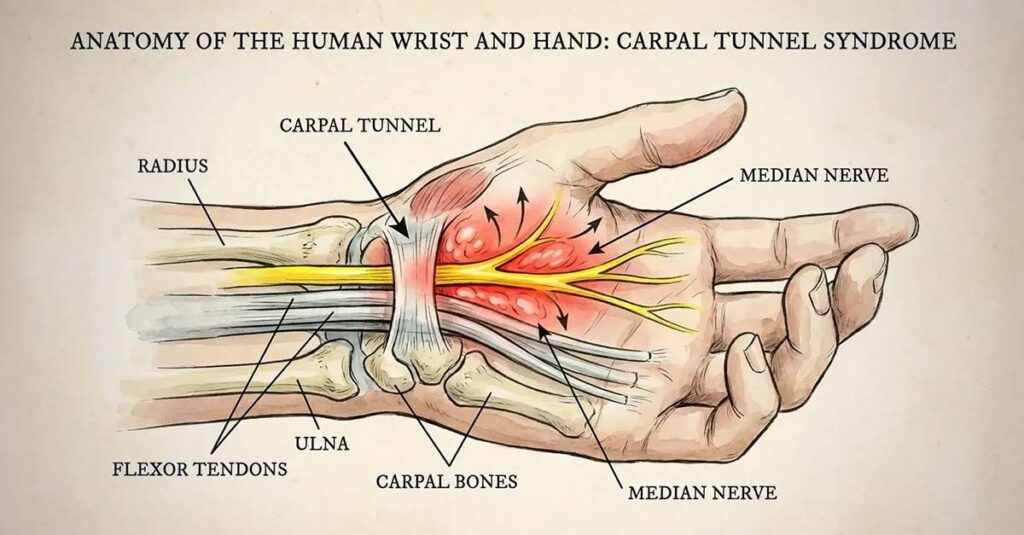
The Median Nerve and Diagnostic Code 8515
The VA Schedule for Rating Disabilities does not contain a line item for “Carpal Tunnel Syndrome” as a named condition. Instead, CTS is evaluated under Diagnostic Code 8515, which addresses paralysis of the median nerve. This classification reflects the VA’s emphasis on functional impairment of the nerve itself—its motor and sensory deficits—rather than the anatomical label of the syndrome. A claim must therefore be constructed around evidence of nerve dysfunction: measurable sensory loss, motor deficits, and objective electrodiagnostic findings.
Major vs. Minor Hand: Why Dominance Matters
One of the most consequential and frequently overlooked distinctions in CTS claims is the VA’s differentiation between the “Major” (dominant) and “Minor” (non-dominant) hand. The VA assigns higher rating percentages to the dominant hand for equivalent levels of nerve impairment, on the basis that dominant-hand dysfunction carries greater impact on occupational function and daily life activities. Hand dominance must be clearly and explicitly identified in all claim documentation.
Illustrative Example: Consider two veterans, both with a clinical finding of Moderate Incomplete Paralysis of the right hand. Veteran A is right-handed; that hand is classified as Major. Veteran B is left-handed; the right hand is classified as Minor. The VA ultimately assigned Veteran A a 30% rating, reflecting the significant impact on the dominant hand’s ability to perform writing, gripping, and daily tasks. Veteran B received a 20% rating for identical medical severity, reflecting the VA’s determination that non-dominant hand impairment is comparatively less disabling for occupational purposes. This example illustrates how hand dominance directly affects the rating outcome for the same clinical presentation.
Incomplete Paralysis: The Functionality Scale
Complete paralysis of the hand is rare in CTS cases. The vast majority of veterans are evaluated along a spectrum of “incomplete paralysis,” which the VA uses to describe graded degrees of sensory and motor deficit. The rating assigned reflects the degree of function lost—ranging from mild (tingling and numbness with largely intact motor function) to severe (significant grip loss, muscle atrophy, and near-total functional impairment). The degree of nerve dysfunction drives the percentage, not the diagnostic label.

Proving the Link: Establishing Service Connection
A current diagnosis of CTS, regardless of severity, does not automatically generate a compensable VA rating for carpal tunnel. The condition must be connected to military service through an established evidentiary framework before the rating schedule is applied. The importance of medical evidence in VA disability claims cannot be overstated when substantiating a nerve condition that is frequently subject to examiner scrutiny.
Three Paths to Connection
Service connection for CTS may be established through three primary pathways, each of which requires a distinct evidence base.
Direct Service Connection
Direct service connection is established when evidence demonstrates that the veteran’s CTS was caused by military duties. This pathway is particularly relevant to veterans whose Military Occupational Specialty (MOS) involved repetitive hand motions, sustained vibration exposure, or heavy manual labor—including mechanics, administrative personnel, signal corps, and machine gunners. Service treatment records reflecting wrist complaints, splint prescriptions, or orthopedic evaluations during active duty are foundational to this pathway.

Secondary Service Connection
Secondary service connection applies when CTS develops as a result of another service-connected condition. Conditions associated with increased CTS incidence include diabetes mellitus, hypothyroidism, rheumatoid arthritis, and amyloidosis. Veterans who use assistive devices such as canes or crutches due to service-connected lower extremity conditions may also develop CTS as a direct result of altered weight-bearing through the upper extremities. When a service-connected condition is the proximate cause of CTS, the carpal tunnel claim may be rated independently under the secondary service connection framework.
Aggravation of Pre-Existing Conditions
Veterans who entered military service with documented mild wrist abnormalities are not automatically disqualified from compensation. Under the aggravation doctrine, the VA recognizes service connection when military service demonstrably worsened a pre-existing condition beyond its natural progression. Entrance examination records noting pre-existing wrist findings, combined with service treatment records and post-separation diagnostic studies showing accelerated deterioration, establish the evidentiary basis for an aggravation claim.
EMG and Nerve Conduction Studies: The Gold Standard
Electromyography (EMG) and Nerve Conduction Velocity (NCV) studies are the objective diagnostic standard for CTS claims. These tests measure the speed and amplitude of electrical signals transmitted through the median nerve; slowed conduction velocity and prolonged distal latency values provide quantifiable evidence of nerve compression. For ratings above the minimum 10%, electrodiagnostic evidence is effectively required. Subjective symptom reports do not independently establish the severity threshold needed for moderate or higher ratings.

Cracking the Code: How Percentages Are Assigned
Once service connection is established, the rating percentage is determined by matching the veteran’s documented symptoms and objective findings to the criteria defined under Diagnostic Code 8515. A VA rating for carpal tunnel is assigned based on the degree of functional impairment, not the diagnosis itself.
VA Rating Tiers for Median Nerve Impairment (Diagnostic Code 8515)
| Paralysis Level | Dominant Hand (Major) Rating | Non-Dominant Hand (Minor) Rating | Key Symptoms |
| Complete Paralysis | 70% | 60% | Hand deviated away from midline; thenar muscle atrophy; inability to form a fist or oppose thumb. |
| Severe Incomplete | 50% | 40% | Considerable loss of motor and sensory function; significant difficulty gripping or pinching. |
| Moderate Incomplete | 30% | 20% | Noticeable functional loss; frequent object dropping; consistent pain with use. |
| Mild Incomplete | 10% | 10% | Tingling, numbness, pain upon motion; motor function largely intact. |
Interpreting the Percentage Tiers
The rating tiers reflect discrete clinical thresholds, and movement between them requires documented changes in both subjective symptoms and objective findings. The specific symptoms corresponding to each tier are captured through standardized evaluation forms; a properly completed DBQ for securing VA benefits ensures the examining provider records the data points the VA requires to assign the correct percentage.
Mild to Moderate: The 10–30% Range
The majority of veterans with CTS receive ratings in the 10–30% range. Mild incomplete paralysis—characterized by intermittent tingling, numbness in the median nerve distribution, and pain upon motion with intact motor function—typically corresponds to a 10% rating. Moderate incomplete paralysis involves a more substantive functional picture: consistent pain during use, measurable grip strength reduction, and the frequent inability to maintain hold on objects.
Illustrative Example: A veteran at the mild (10%) level experiences paresthesias during sustained gripping or typing but retains the ability to perform most daily tasks without interruption. A veteran at the moderate (30% Major) level experiences frequent, unpredictable grip failures—dropping objects, being unable to sustain tool use—with EMG studies confirming moderate median nerve slowing. The distinction between these two presentations is corroborated by both electrodiagnostic findings and functional assessment documentation.
Severe to Complete: When Function Stops
Ratings of 50% or 70% are reserved for severe and complete paralysis presentations, respectively. Severe incomplete paralysis involves considerable loss of both motor and sensory function, with significant grip and pinch strength reduction documented on objective testing. Complete paralysis—rated at 70% for the major hand—is characterized by thenar muscle atrophy, wrist deviation, and the inability to form a fist or perform opposition. These presentations are clinically uncommon in CTS cases and require robust objective evidence.
The Bilateral Factor
Veterans with CTS affecting both hands are subject to the VA’s bilateral factor calculation. Under this provision, the VA combines the individual ratings for each extremity using the combined ratings formula, then adds 10% of that combined value to the total. This adjustment reflects the VA’s recognition that bilateral upper extremity impairment carries substantially greater impact on occupational function and daily living than single-hand involvement.
Pain vs. Paralysis
Veterans whose nerve impairment does not meet the clinical threshold for a higher paralysis-based rating retain a regulatory pathway to compensation based on documented pain during motion.

The Painful Motion Rule (38 CFR § 4.59)
Under 38 CFR § 4.59, the VA is required to recognize painful motion as a basis for at least the minimum compensable rating for the affected joint or extremity. When wrist motion produces pain—regardless of whether the range of motion measurement falls within normal parameters—the minimum 10% rating is generally applicable. This provision is independent of electrodiagnostic severity and applies even in cases where nerve conduction studies indicate only mild slowing.
Documenting Functional Loss
Clinical test results establish the presence and severity of nerve impairment, but functional loss documentation communicates the real-world impact of the condition. The VA’s rating criteria under 38 CFR § 4.40 and § 4.45 specifically address functional loss due to pain, weakness, and incoordination. Concrete descriptions of how the condition interferes with specific activities—keyboarding, driving, personal care tasks, occupational duties—provide the VA rater with the contextual evidence needed to evaluate disability beyond numerical measurements alone.
Life After the Knife: Post-Surgical Ratings
Many veterans with service-connected CTS undergo carpal tunnel release surgery to decompress the median nerve. Understanding how this procedure affects the VA disability rating for carpal tunnel after surgery is essential to protecting benefits during the recovery period and beyond.

Temporary Convalescence Benefits and the 100% Temporary Rating
When a veteran undergoes surgery for a service-connected condition and recovery requires at least one month of convalescence or results in severe immobilization, the VA may assign a temporary 100% rating under Diagnostic Code 5055. This temporary rating reflects the period during which the veteran is functionally incapacitated by the surgical recovery process rather than the underlying nerve condition.
Timeline for Re-Evaluation
The temporary 100% surgical rating is time-limited, typically lasting one to three months depending on the treating physician’s documented recovery timeline. Following the convalescence period, the VA schedules a re-evaluation to assess residual symptoms and assign a permanent post-surgical rating. Post-surgical examinations should thoroughly document any persistent sensory deficits, grip strength limitations, or pain that remains after recovery.
Long-Term Adjustments and the Minimum Rating Rule
When surgery produces complete symptom resolution, the VA may reduce the rating to reflect the improved condition. However, complete resolution is clinically uncommon. Veterans who retain residual symptoms—persistent numbness, grip weakness, pillar pain at the incision site—generally retain at least the minimum compensable rating. A rating is not typically reduced to 0% unless the veteran is entirely asymptomatic and all objective measurements fall within normal parameters.
Scars and Residual Symptoms
Carpal tunnel release surgery involves a palmar incision, and the resulting scar may generate an additional rating if it is painful or unstable. Diagnostic Code 7804 governs painful or unstable surgical scars, and a separately documented scar condition may be rated concurrently with any residual nerve impairment. Pillar pain—a common post-surgical complaint involving aching at the base of the thenar and hypothenar eminences—and persistent grip strength loss are additional residual findings that may support supplemental or increased ratings following surgery.
Building a Well-Documented Claim
Accurate knowledge of the medical criteria is a necessary but insufficient foundation for a well-supported CTS claim. The evidentiary record must be constructed with equivalent rigor. The top seven reasons VA disability claims get denied frequently include evidentiary gaps that a structured pre-submission review can identify.

The Evidence Stack
The following categories of documentation are typically relevant to a well-supported CTS claim:
- Current Diagnosis: Medical records from within the last 12 months confirming CTS
- Objective Testing: EMG or Nerve Conduction Study results, essential for ratings above 10%
- Nexus Documentation: A medical opinion linking the current CTS to military service, if not established through a presumptive or direct pathway
- DD-214: Proof of service and MOS detail
- Statement in Support of Claim (VA Form 21-4138): A personal account of symptom history and functional impact
- Lay Witness Statements: Statements from spouses or fellow service members describing observed symptoms and functional limitations
- Service Treatment Records: Records documenting any in-service complaints, evaluations, or treatment of the wrist or hand
Personal Statements and Lay Evidence
VA Form 21-4138 provides the veteran with an opportunity to describe the daily functional impact of the condition in concrete, specific terms. Lay witness statements from spouses, family members, or fellow service members who have directly observed grip failures, nightly symptom interruption, or limitations in daily tasks contribute lay evidence that supplements clinical documentation.
Reviewing Service Treatment Records
Service treatment records may contain entries—wrist splint prescriptions, medic visit notes, complaints of hand numbness during field operations—that establish the in-service origin of the condition. Each relevant entry contributes to the evidentiary chain connecting the current diagnosis to active duty service.
The C&P Examination
The Compensation and Pension (C&P) examination is the VA’s primary tool for assessing current severity. According to the VA, this examination is used to document diagnosis, symptom severity, and functional limitations, which the VA then applies to the rating criteria.

Phalen’s and Tinel’s Tests
During the C&P examination, the examiner will typically perform Phalen’s maneuver (sustained wrist flexion to reproduce paresthesias) and Tinel’s sign (percussion over the carpal tunnel to elicit a tingling response). These are standard clinical tests for CTS. Per VA policy, range of motion measurements and pain onset are documented at the point at which symptoms are first elicited—not at the maximum range the veteran can reach through pain.
Illustrative Example: During the examination, the examiner asks the veteran to flex the wrist. Pain begins at 20 degrees of flexion, but the veteran is physically capable of reaching 45 degrees. If flexion proceeds to 45 degrees without communication of earlier pain onset, the examiner records a normal or near-normal range of motion finding. When pain onset at 20 degrees is communicated to the examiner at that moment—”It hurts right there”—the examiner documents limited range of motion due to pain, directly supporting the application of 38 CFR § 4.59. This example illustrates how the accuracy of pain onset communication during the examination affects the clinical record.
Responding to Denials and Low Ratings
A denial or a rating that does not reflect clinical reality is not a final determination. According to the VA, several review pathways are available to veterans who disagree with a rating decision.
Appeal Pathway Overview
| Appeal Lane | Best Used When… | What Is Submitted |
| Higher-Level Review (HLR) | The VA is believed to have made an error based on existing evidence. | No new evidence; a senior rater reviews the existing file. |
| Supplemental Claim | New and relevant evidence not previously considered is available. | New medical records, updated EMG results, new nexus documentation, or additional lay statements. |
| Board Appeal | The HLR or Supplemental decision is disputed and a more formal review is sought. | May involve a hearing or direct review; typically involves longer processing timelines. |
Higher-Level Reviews vs. Supplemental Claims
A Higher-Level Review is appropriate when the evidentiary record is complete but the rating decision is believed to reflect a factual or regulatory error. No new evidence may be submitted through this pathway. A Supplemental Claim is the appropriate vehicle when new and relevant evidence—such as an updated electrodiagnostic study, a private medical opinion, or a newly completed DBQ—was not part of the original claim record.
The Role of Independent Medical Opinions
When a C&P examiner’s evaluation does not document specific functional findings—grip strength measurement, wrist range of motion, detailed sensory mapping—a private Disability Benefits Questionnaire (DBQ) completed by an independent licensed provider can address those evidentiary gaps. An independent medical opinion that specifically addresses the criteria of Diagnostic Code 8515, documents painful motion under 38 CFR § 4.59, and provides objective electrodiagnostic correlation may supply the clinical foundation that a prior denial lacked.
Intent to File and Effective Dates
According to the VA, submitting an Intent to File (VA Form 21-0966) establishes a potential effective date while evidence is being assembled. Per VA policy, if a complete claim is submitted within one year of the Intent to File date, the effective date—and the back pay calculation that depends on it—is preserved from the original filing date.
Independent Medical Documentation for CTS Claims
CTS claims frequently fall short not because the condition lacks merit, but because the medical documentation does not capture the specific clinical language and objective findings the VA’s rating schedule requires. A C&P examination that does not quantify grip strength, measure wrist range of motion under the painful motion standard, or map the precise sensory deficit distribution along the median nerve may leave the evidentiary record incomplete.
REE Medical coordinates access to independent, licensed medical professionals experienced in completing VA-standardized DBQs that accurately reflect the full clinical scope of median nerve impairment. These providers document findings consistent with the criteria of Diagnostic Code 8515—addressing paralysis severity, functional loss, and painful motion in objective, measurable terms. Veterans whose current rating may not fully reflect the severity of their conditions can learn more about available options for submitting additional medical documentation. Veterans can learn more about coordinating a comprehensive evaluation by contacting REE Medical.
Final Thoughts
A VA rating for carpal tunnel that accurately reflects a veteran’s functional impairment depends on more than the diagnosis itself. It requires a precise understanding of Diagnostic Code 8515, documented objective evidence of median nerve dysfunction, clear identification of hand dominance, and clinical documentation that addresses each dimension of functional loss—including pain during motion, grip strength deficits, and sensory impairment. The gap between a 10% and a 30% rating is not always a matter of medical severity; it is frequently a matter of how thoroughly the evidence record captures that severity. Thorough, objective medical documentation is the mechanism through which the VA can evaluate the full impact of the condition accurately.
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (VA). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veterans Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.


