
VA Rating for High Blood Pressure: What Every Veteran Needs to Know
Hypertension is one of the most prevalent chronic conditions in the veteran population, affecting more than 2.5 million veterans and representing one of the most commonly service-connected disabilities according to the U.S. Department of Veterans Affairs. Despite its prevalence, many veterans receive ratings that do not accurately reflect the severity of their condition—or receive denials where the medical evidence may not fully reflect the severity of the condition.
This guide breaks down the regulatory framework governing a VA rating for high blood pressure, the specific evidentiary standards that determine rating percentages, and the documentation strategies that produce the most accurate clinical picture for VA evaluation. Each section is designed to close the gap between the clinical reality of living with hypertension and what the medical record captures for rating purposes.
TL;DR
- The VA rates hypertension from 10% to 60% under Diagnostic Code 7101, based primarily on diastolic blood pressure readings documented across multiple clinical appointments
- Continuous medication for blood pressure control automatically qualifies for a minimum 10% rating, regardless of how effectively that medication manages the condition
- Multiple blood pressure readings over time are required to establish the patterns the VA uses for rating decisions
- Secondary conditions—including heart disease, kidney disease, and stroke—may each qualify for separate ratings that combine with the hypertension rating
- Medication side effects constitute legitimate functional limitations relevant to the overall disability picture
- Thorough documentation of symptoms and daily functional impact is central to an accurate rating outcome
- Initial claims require establishing service connection; increase claims focus on demonstrating that an already-rated condition has worsened

Understanding How the VA Rates High Blood Pressure
The VA classifies hypertension under Diagnostic Code 7101 as a cardiovascular disability. This classification determines the entire evaluative framework for the condition, producing ratings from 10% to 60% depending on documented blood pressure levels and treatment requirements. A VA rating for high blood pressure is not assigned based on whether elevated readings exist—it is assigned based on how severe those elevations are, how consistently they appear in the medical record, and what level of medical intervention is required to manage the condition.
The VA’s evaluation extends beyond blood pressure numbers. The importance of medical evidence in VA disability claims is particularly significant in hypertension cases, where the completeness and consistency of the clinical record directly shapes the rating outcome. The VA examines severity, the presence of complications, and the functional impact on daily life—all of which must be reflected in the documentary record to influence the rating.
Blood Pressure Numbers and Rating Percentages
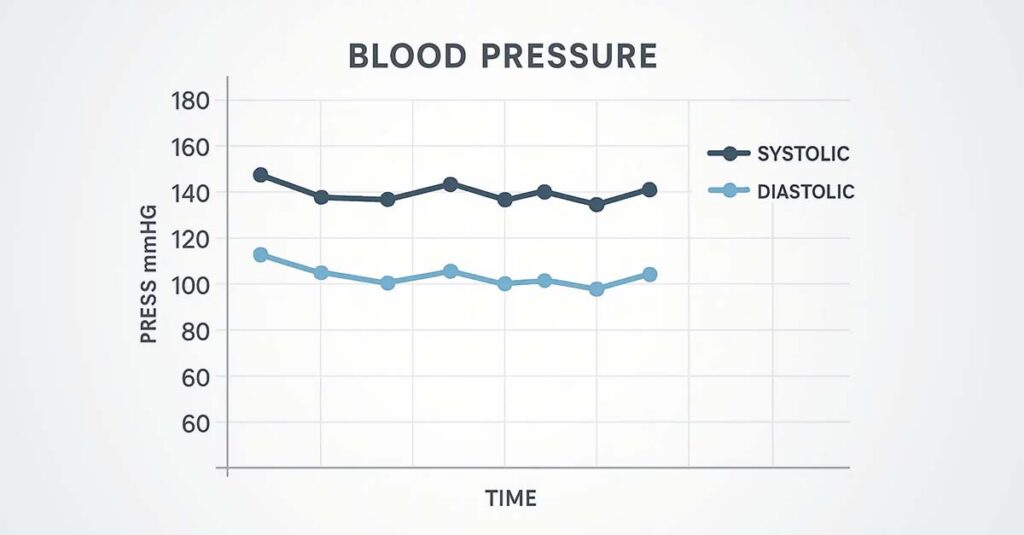
The VA assigns hypertension ratings based on diastolic blood pressure as the primary metric, with systolic pressure as an alternative basis at lower rating tiers. The term “predominantly” in the rating criteria is clinically significant—the VA is looking for consistent patterns across multiple readings, not isolated elevated measurements.
| VA Disability Rating | Diastolic Pressure (mmHg) | Systolic Pressure (mmHg) |
| 10% | 100 or higher (predominantly) | 160 or higher (predominantly) |
| 20% | 110 or higher (predominantly) | 200 or higher (predominantly) |
| 40% | 120 or higher (predominantly) | N/A |
| 60% | 130 or higher (predominantly) | N/A |
A critical component of the rating framework: continuous medication for blood pressure control automatically qualifies for a minimum 10% rating under VA regulations, regardless of how effectively that medication controls the condition. The VA’s position is that requiring daily medication to manage a chronic condition represents an ongoing disability, even when treatment produces normal readings. This provision prevents veterans from receiving a 0% rating solely because treatment is effective.
For current monthly compensation amounts by rating percentage, VA Disability Compensation Rates provides the most current figures.
Why Multiple Readings Matter
Blood pressure fluctuates based on stress, medication timing, physical activity, and circadian patterns. A single elevated reading does not establish hypertension for rating purposes, and a single normal reading does not refute it. The VA requires documentation of blood pressure patterns across multiple clinical appointments to establish what level predominantly characterizes the condition.
According to Sean Kendall Law, the VA requires blood pressure measurements on at least three separate days, with a minimum of two readings per day taken under appropriate clinical conditions. Informal readings—such as those taken at pharmacy kiosks—do not satisfy this standard. Professionally documented measurements from medical appointments carry the evidentiary weight the VA requires.
A veteran evaluated for a hypertension claim submitted records from only two medical appointments and received an inaccurate rating. After accumulating 18 months of consistent readings from a primary care physician and cardiologist that consistently reflected diastolic pressures between 120–125 mmHg, the clinical pattern supported a 40% rating. The VA ultimately assigned the higher rating based on the updated evidentiary record. The additional documentation did not change the underlying condition—it provided the longitudinal pattern the VA needed to assign an accurate rating.
Essential Medical Evidence
Medical evidence is the foundation of any hypertension rating determination. The VA evaluates the completeness, consistency, and clinical specificity of the record. Understanding what evidence is needed for a disability claim clarifies which documentation categories carry the most weight in a hypertension evaluation.
Essential Evidence Checklist:
- Multiple blood pressure readings from different appointments over 3–6 months
- Complete medication list with dosages and start dates
- Documentation of medication side effects and their functional impact
- Records showing blood pressure patterns before and after medication initiation
- Emergency department visits related to blood pressure crises
- Specialist consultations (cardiology, nephrology, ophthalmology as applicable)
- Service medical records reflecting any blood pressure documentation during active duty
Building Strong Medical Documentation
The medical record must reflect the full clinical picture of the hypertension—not simply a series of blood pressure measurements. Complete medication history, including treatment trials, adjustments, and discontinuations due to side effects or inadequate control, provides the VA with context for understanding disease severity and management complexity.
Secondary conditions and complications that have developed as a consequence of hypertension—including cardiac, renal, or ophthalmologic involvement—are clinically relevant and must appear in the record. Functional limitations attributable to the condition or its treatment, including activity restrictions, dizziness, fatigue, and sleep disruption, need to be documented with specificity to inform the VA’s evaluation of overall disability impact.

Establishing Service Connection
Per VA guidelines, three pathways exist for establishing service connection for hypertension. Direct service connection requires documentation of blood pressure issues in service treatment records, establishing that the condition originated during active duty. Secondary service connection applies when hypertension developed as a downstream consequence of another service-connected condition—chronic stress associated with service-connected PTSD has an established physiological relationship with hypertension development.
As noted by Hill & Ponton, hypertension is a presumptive condition for veterans with Agent Orange exposure, and it is also presumptive when it manifests to a compensable degree—10% or greater—within one year of discharge from active duty.
The Disability Benefits Questionnaire
The hypertension Disability Benefits Questionnaire (DBQ) is the standardized clinical form through which the examining physician translates medical findings into the specific format the VA rating authority applies. The DBQ captures blood pressure readings, medication requirements, side effects, and functional impact in a structured format aligned with the rating criteria. Understanding the VA DBQ process clarifies how this document functions as the primary interface between clinical findings and rating outcomes. A DBQ completed by a provider experienced with disability-focused documentation ensures the rating authority has the specific information required for an accurate determination.
Secondary Conditions That Affect Your Rating
Hypertension exerts sustained physiological stress on multiple organ systems, and the secondary conditions that develop as a result may each qualify for independent disability ratings under VA regulations. These ratings combine with the primary hypertension rating using VA combined ratings methodology, producing a higher total disability percentage than the hypertension rating alone.
Secondary conditions must be documented with the same clinical specificity as the primary condition to support accurate independent ratings.
Heart Disease and Cardiac Complications
Chronic hypertension increases cardiac workload and accelerates atherosclerotic disease, producing conditions including coronary artery disease, heart failure, and cardiac arrhythmias. These conditions carry substantial disability ratings—potentially 30%, 60%, or 100% depending on documented severity and functional impact. Cardiac testing including electrocardiograms, stress tests, echocardiograms, and cardiac catheterization provides the objective data required for these ratings. Symptoms including chest pain, dyspnea, and exercise intolerance require clinical evaluation both for treatment purposes and for disability documentation.
Kidney Disease
Hypertensive nephrosclerosis—kidney damage resulting from sustained elevated blood pressure—is frequently asymptomatic in its early stages, making regular laboratory monitoring critical for detection. The VA rates chronic kidney disease based on measured reduction in renal function, with higher ratings assigned as glomerular filtration rate declines. Creatinine levels, GFR measurements, and urinalysis results constitute the objective evidentiary foundation for kidney disease ratings.
Vision and Neurological Complications
Hypertensive retinopathy and stroke represent serious end-organ complications of uncontrolled hypertension that carry independent rating potential. Vision changes require ophthalmologic examination and documentation of retinal findings. Stroke history requires neuroimaging and neurological assessment. Both categories of complications can produce significant independent ratings that combine with the primary hypertension evaluation.
Secondary Condition Rating Reference:
| Secondary Condition | Typical VA Rating Range | Key Documentation |
| Coronary Artery Disease | 30–100% | Cardiac catheterization, stress tests, EKG |
| Heart Failure | 30–100% | Echocardiogram, ejection fraction, functional capacity |
| Chronic Kidney Disease | 0–100% | Creatinine levels, GFR, dialysis records |
| Hypertensive Retinopathy | 0–100% | Eye exams, visual field tests, retinal photographs |
| Stroke | 10–100% | MRI/CT imaging, neurological assessments |

Filing: Initial Claims and Increase Claims
Understanding the distinction between an initial claim and an increase claim is important because the evidentiary requirements differ materially between the two. Initial claims require establishing that a ratable condition exists and that it is connected to military service. Increase claims require demonstrating that an already service-connected condition has worsened beyond what the current rating reflects.
Initial Claims
An initial hypertension claim requires three evidentiary components: a current diagnosis of hypertension supported by clinical documentation, evidence of service connection through one of the three recognized pathways, and a medical opinion establishing the relationship between service and the current condition when that relationship is not self-evident from the record.
The service connection element is frequently the most challenging component for veterans whose hypertension developed gradually after discharge or was not well-documented during service. When service treatment records do not reflect blood pressure issues, alternative forms of evidence—including lay statements and independent medical opinions—may support the connection.
Increase Claims
A veteran whose hypertension has worsened since the prior rating decision may be eligible for a higher rating. Worsening may be reflected through consistently higher blood pressure readings, escalation to stronger or additional medications, or the development of complications not previously documented. The VA compares current clinical findings against the baseline established at the prior rating.
Per VA guidance, veterans may request a VA disability rating increase when medical evidence reflects genuine deterioration in the rated condition. An increase claim filed during a period of temporary blood pressure fluctuation without supporting longitudinal evidence may not reflect the stable worsening required for a durable rating increase.
As noted by Hill & Ponton, the average VA rating for hypertension tends to fall in the 0–10% range, reflecting the most common presentation of medication-controlled blood pressure with moderate elevation.

Common Documentation Mistakes
Many hypertension claims that reflect genuine disability do not produce accurate ratings because of documentation deficiencies rather than clinical ones. Understanding the top reasons VA disability claims are denied helps identify the most common evidentiary gaps before they affect the rating outcome.
Insufficient Pattern Documentation
Submitting a small number of isolated blood pressure readings is one of the most common sources of rating inaccuracy in hypertension claims. The VA’s “predominantly” standard requires longitudinal clinical documentation—readings spread across multiple appointments over months—that establishes a consistent blood pressure range rather than episodic elevations.
Incomplete medication histories are a related documentation gap. The VA reviews not only which medications a veteran currently takes, but what treatments have been tried, what dosage adjustments have been made, and what side effects have been experienced. This information provides critical context for evaluating disease severity and management complexity.
Service Connection Gaps
Veterans whose hypertension is not documented in service treatment records face a higher evidentiary burden for service connection. The absence of in-service documentation does not preclude a successful claim, but it requires alternative evidence—post-service records demonstrating early onset, independent medical opinions, or lay statements—to bridge the gap between service and the current diagnosis.
Medication Compliance Misunderstandings
A prevalent misconception is that well-controlled blood pressure undermines a disability claim. Under VA regulations, continuous medication for hypertension qualifies for a minimum 10% rating regardless of treatment effectiveness. Effective treatment does not eliminate the disability—it reflects ongoing management of a chronic condition. Discontinuing prescribed medication before a VA examination is medically dangerous and may raise questions about treatment compliance that complicate the claim.
How Medications Affect Your Rating
Medication type, dosage complexity, and side effects are all relevant to the VA’s overall disability assessment. The total management burden of hypertension—not only the blood pressure readings themselves—informs how the condition affects daily functioning.
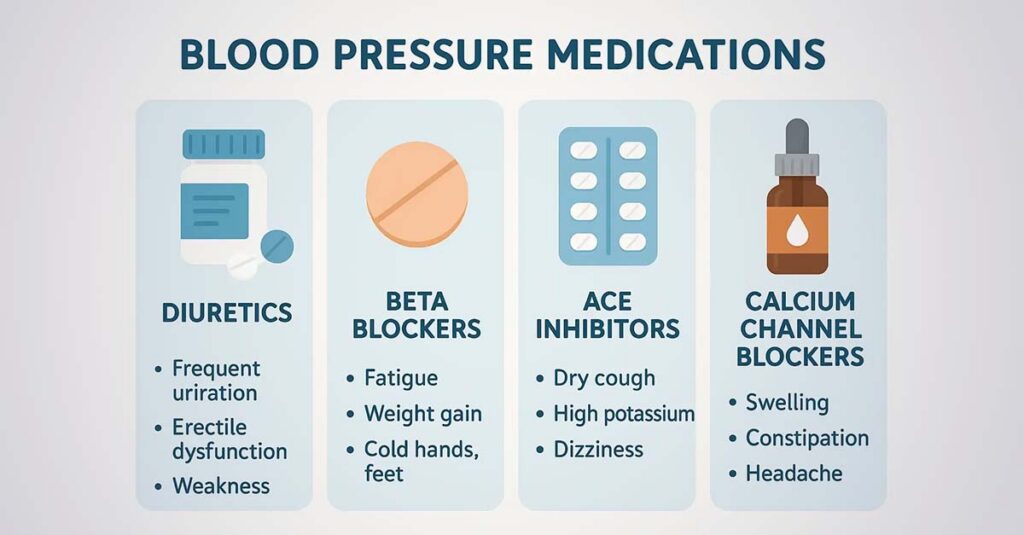
Beta Blockers and ACE Inhibitors
Beta blockers commonly produce fatigue, exercise intolerance, and reduced physical stamina. Veterans who experience meaningful reduction in physical capacity due to beta blocker therapy have a functional limitation directly attributable to the service-connected condition and its treatment. ACE inhibitors commonly produce a persistent dry cough, dizziness, and fatigue. Both medication classes have functional implications that extend beyond blood pressure control and are most useful when documented in the medical record with specific examples of their daily impact.
Diuretics and Quality of Life
Thiazide and loop diuretics produce frequent urination, nocturia, electrolyte imbalances, muscle cramping, and orthostatic dizziness—consequences that disrupt work performance, sleep quality, and daily functioning. A veteran whose diuretic regimen produces nocturia four to five times per night experiences measurable sleep disruption with daytime functional consequences. When these side effects are documented with clinical specificity—including frequency, duration, and functional impact—they become part of the evidentiary record the VA reviews.
A veteran with a 10% hypertension rating prescribed a diuretic that produced urinary frequency every 30–45 minutes during the day and nocturia four to five times per night documented the condition’s impact on job performance and sleep quality. When an increase claim was filed, the functional limitations from medication side effects were part of the evidence the VA reviewed. The VA ultimately assigned a 20% rating based on the totality of the documented evidence.
Complex Medication Regimens
Multi-drug therapy for blood pressure control reflects a condition that has not been adequately managed by simpler interventions. Combination therapy indicates greater disease severity, more complex daily management requirements, and a higher cumulative side effect burden. Documentation of a multi-drug regimen—including each medication, dosage, prescribing indication, and associated side effects—provides the VA with a more complete picture of the condition’s overall functional impact.
Medication Documentation Checklist:
- Complete list of all blood pressure medications with dosages
- Start dates for each medication
- Documentation of any medication changes or adjustments
- Side effects experienced from each medication
- Functional impact of side effects on daily activities
- Medications tried but discontinued due to side effects or inadequate control
- Frequency of medication monitoring appointments

Documentation Strategies That Produce Accurate Ratings
Effective documentation combines objective clinical data with specific, functional descriptions of how the condition affects daily life. The VA examiner reviewing a claim file should be able to identify from the record both the measurable severity of the condition and its real-world impact on the veteran’s functioning.
Symptom Tracking
A consistently maintained symptom log provides longitudinal evidence of functional impact that complements objective blood pressure readings in the medical record. Symptom entries are most useful when they include specific functional consequences—not simply notation that a symptom occurred.
Daily Symptom Log Template:
- Date and time
- Blood pressure reading (if clinically obtained)
- Symptoms experienced (headache, dizziness, fatigue, chest discomfort)
- Severity rating (1–10 scale)
- Activities affected or avoided
- Medication timing and any observed side effects
- Duration of symptoms
- Factors that improved or worsened the episode

Clinical Appointment Documentation
Each medical appointment is an opportunity to document the current state of the condition and its functional impact. Describing symptoms with specificity—quantifying how far walking tolerance has declined, how fatigue affects work performance, or how dizziness affects daily activities—produces the kind of functional documentation that informs an accurate disability rating. Functional limitations documented in the clinical note by the treating physician carry evidentiary weight with the VA that lay statements alone cannot replicate.
Building the Evidence File
A well-organized evidence file presents the longitudinal history of the condition in a format the rating authority can review clearly. Chronological organization of records allows the progression of the condition—onset, treatment history, worsening, and current status—to be followed in sequence. A concise summary identifying key blood pressure readings, medication requirements, and documented functional limitations reduces the risk that critical evidence is overlooked.
Accurate Documentation Through REE Medical
C&P examinations may not capture the full scope of a veteran’s hypertension—particularly when readings on the day of examination do not reflect the predominantly elevated pattern documented across months of clinical appointments, or when medication side effects and functional limitations have not been explicitly addressed in the clinical record.
REE Medical connects veterans with independent, licensed healthcare professionals who complete hypertension DBQs and medical evaluations with the clinical thoroughness that an accurate VA rating for high blood pressure determination requires. Documentation coordinated through REE Medical is objective, VA-compliant, and completed by providers experienced in disability-focused clinical documentation standards—capturing blood pressure patterns, medication requirements, side effects, and functional limitations in the format the VA applies. REE Medical operates on a flat-rate model with transparent pricing; no percentage of future benefits is taken.
Veterans can learn more about coordinating independent medical documentation by contacting REE Medical for a complimentary informational consultation.
Final Thoughts
A VA rating for high blood pressure that accurately reflects disease severity requires documentation that captures the condition across its full clinical scope: consistent blood pressure measurements over time, a complete medication and side effect history, functional limitations attributable to the condition and its treatment, and the secondary complications that have developed as a result of chronic hypertension.
The rating framework under Diagnostic Code 7101 is objective and quantifiable, but only when the medical record contains the specific data the criteria require. Continuous medication automatically qualifies for a minimum 10% rating. Diastolic readings consistently above 120 mmHg are associated with a 40% rating. Secondary conditions that develop from hypertension carry independent ratings. Each of these components depends entirely on what is documented in the clinical record.
Veterans who understand how the VA evaluates hypertension, what evidence the rating criteria require, and how to document the full functional impact of the condition are better positioned to receive compensation that reflects the actual burden of their service-connected disease.
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (“VA”). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veteran’s Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.


