VA Disability Rating for Heart Stent: How the VA Evaluates Heart Conditions
A heart stent is a life-saving intervention—but it is not what the Department of Veterans Affairs rates for disability compensation purposes. The VA evaluates the underlying cardiovascular disease, the functional limitations it produces, and the objective data that quantifies how severely heart function has been compromised. For veterans navigating this process, understanding the distinction between the surgical procedure and the residual disability is the foundation of an accurate claim.
This guide provides an overview of the diagnostic codes, clinical evaluation criteria, and documentation elements the VA may reference when reviewing disability claims involving heart stent–related conditions. The purpose is to help illustrate how medical findings and clinical records can relate to the information considered during the VA’s evaluation process.
TL;DR
For veterans who need the critical framework before reading further:
- It is not the stent: The VA rates the underlying Ischemic Heart Disease (IHD), not the presence of the device itself.
- Function is the metric: Ratings are determined by METs (Metabolic Equivalents) and LVEF (Left Ventricular Ejection Fraction) results.
- Temporary 100%: Veterans are entitled to a temporary 100% rating for three months following stent surgery when the condition is service-connected.
- Presumptive service connection: Veterans exposed to Agent Orange or toxins covered under the PACT Act may qualify for automatic service connection for IHD.
- Accurate symptom reporting matters: Describing symptoms as they occur and their impact on daily functioning helps ensure the medical record reflects the Veteran’s current clinical picture.
Pre-Filing:
- A documented diagnosis related to an ischemic heart condition
- Medical evidence describing any relevant exposures or service‑connected factors
- Recent echocardiogram results stating LVEF percentages
- Stress test findings including METs levels, if applicable
- Documented symptoms such as shortness of breath, fatigue, or chest discomfort
It Is Not the Stent, It Is the Function
Many veterans entering the claims process assume that cardiac surgery automatically produces a high disability rating. The VA’s evaluation framework does not operate on that basis. What matters is the residual functional impact of the underlying disease—primarily Ischemic Heart Disease—after all treatment has been applied. The surgical intervention is a data point in the medical history, not the basis of the rating.
Ischemic Heart Disease Explained
Coronary Artery Disease (CAD) and Ischemic Heart Disease describe conditions in which reduced blood flow to the heart muscle compromises its function. VA disability evaluations for heart‑related conditions generally consider clinical findings such as cardiac function and the level of exertion at which symptoms occur. A stent procedure is typically documented as part of a Veteran’s medical history, and post‑treatment records may reflect changes in functional capacity. Symptom documentation in follow‑up evaluations helps provide the VA with information about a Veteran’s ongoing clinical picture. For veterans managing the long-term impact of cardiovascular disease, heart health tips for heroes provides context on the lifestyle factors that intersect with ongoing cardiac health.
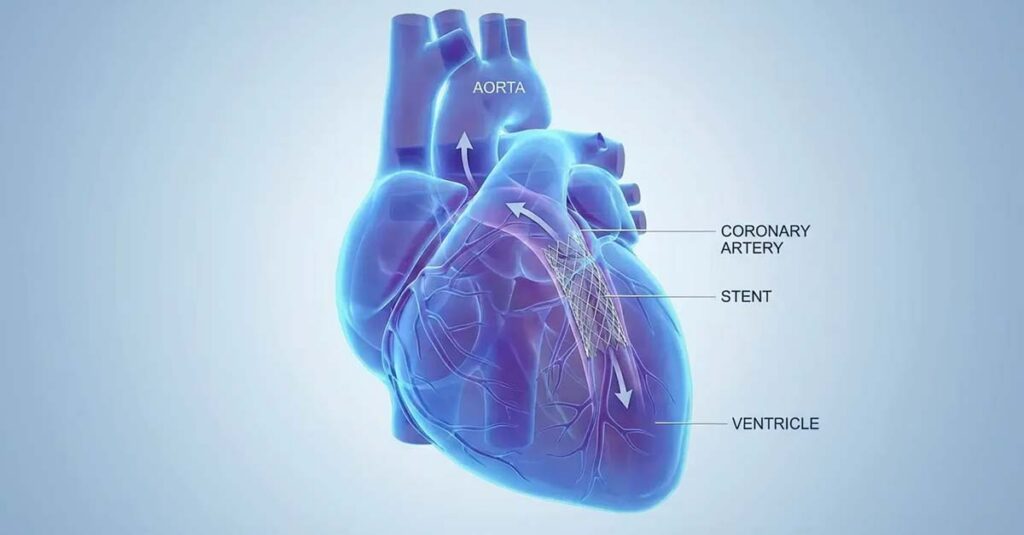
Stents Are Treatments, Not Cures
A coronary stent is a mesh scaffolding device placed within a narrowed artery to maintain patency and restore blood flow. It addresses a mechanical obstruction but does not resolve the underlying atherosclerotic disease process responsible for that obstruction. Chronic heart disease continues to progress after stent placement, and the VA’s rating schedule is calibrated to the functional limitations that persist following treatment—not the absence of further acute events.
Residual Symptoms and the Medical Record
Post-surgical residual symptoms—including angina, dizziness, dyspnea on exertion, and fatigue—are clinically meaningful and directly relevant to the rating determination. When these symptoms are not reported or documented consistently after a procedure, the medical record implies full recovery. VA disability evaluations rely on the medical evidence contained in a Veteran’s record. If ongoing symptoms are not fully documented in clinical notes, the available information may not reflect the severity of the condition.
Proving the Military Caused Your Heart Condition
Service connection is the prerequisite for any VA disability rating. Without an established link between the cardiac condition and military service, the rating process cannot proceed. Three distinct pathways exist through which IHD and related heart conditions may be connected to service.
The Direct Route
Direct service connection applies when a cardiac diagnosis was established during active duty, or when a documented service event created the conditions from which heart disease subsequently developed. This pathway typically requires evidence demonstrating a continuity of symptoms or a clear medical relationship between the in-service occurrence and the current diagnosis.
Presumptive Conditions: Agent Orange and the PACT Act
For veterans who served in Vietnam or in other locations and time periods covered by Agent Orange herbicide exposure, the VA recognizes Ischemic Heart Disease as a presumptive condition. This designation means the VA concedes the service connection without requiring a formal medical nexus opinion, provided the veteran’s service history meets the qualifying criteria. The PACT Act extended similar presumptive frameworks to veterans exposed to burn pit particulate matter and other deployment-era toxins, expanding the population of veterans for whom this pathway applies.
The Secondary Connection
IHD does not always develop as the primary service-connected condition. Cardiovascular disease frequently emerges as a secondary consequence of other rated disabilities—most commonly hypertension, Type 2 diabetes, and PTSD. Each of these conditions places measurable chronic stress on the cardiovascular system. An independent medical opinion establishing that the heart condition is at least as likely as not caused or aggravated by the primary service-connected disability can support a secondary service connection determination by the VA.
Understanding VA Heart Ratings
The VA evaluates Ischemic Heart Disease under Diagnostic Code 7005. Understanding how the rating schedule is structured helps explain how objective cardiac findings are reviewed. This technical framework is the foundation of every accurate va disability rating for heart stent evaluation.
For context on how these rating percentages translate into monthly compensation figures, VA Disability Compensation Rates provides current benefit amounts by combined rating level. For a broader explanation of how individual percentages are calculated and combined, understanding VA disability ratings outlines the methodology in detail.
| Rating | Left Ventricular Ejection Fraction (LVEF) | METs (Workload Capacity) | Other Key Symptoms |
| 100% | Less than 30% | 3.0 METs or less | Chronic Congestive Heart Failure |
| 60% | 30% to 50% | 3.1 to 5.0 METs | More than 2 episodes of incapacitation per year |
| 30% | 50% to 55% | 5.1 to 7.0 METs | Evidence of cardiac hypertrophy or dilation |
| 10% | More than 55% | 7.1 to 10.0 METs | Requires continuous medication |
Diagnostic Code 7005 Breakdown
The VA assigns a single rating based on the predominant disability picture—meaning the most severe combination of objective test results and documented symptoms determines the rating level. Veterans are not required to satisfy every criterion within a tier; meeting any one of the defining characteristics for a given level is sufficient to trigger that rating.
The 100% Rating
A 100% rating applies when the medical record documents chronic congestive heart failure, an LVEF below 30%, or a workload capacity at or below 3.0 METs. This level reflects near-total cardiovascular limitation—a state in which minimal physical activity produces symptomatic distress.
The 60% Rating
A 60% rating applies when LVEF falls between 30% and 50%, or when workload capacity registers between 3.1 and 5.0 METs. Veterans who have experienced more than two episodes of incapacitation requiring bed rest or hospitalization within a calendar year also fall within this rating tier.
The 30% Rating
A 30% rating is assigned when LVEF is between 50% and 55%, or workload capacity falls in the 5.1 to 7.0 METs range. Imaging evidence of cardiac hypertrophy or dilation—reflected on X-ray or electrocardiogram—also corresponds to this rating level.
The 10% Rating
The 10% rating represents the baseline compensable threshold. It applies when a veteran requires continuous cardiac medication, or when workload capacity falls between 7.1 and 10.0 METs with an LVEF above 55%. While this represents the least severe compensable tier, it establishes service connection and preserves the claim for future review if the condition progresses.
Why METs Matter More Than You Think
Metabolic Equivalents are frequently the determinative factor in cardiac disability ratings, yet many veterans entering the claims process are unfamiliar with the metric. Because METs directly correlate to the functional thresholds that define each rating level under Diagnostic Code 7005, the accuracy of METs documentation in the medical record plays an important role in how functional limitation is reflected. This makes accurate va disability rating for heart stent evaluation dependent on how precisely stress test data reflects real-world functional capacity.

Defining Metabolic Equivalents
A MET represents the metabolic energy cost of a physical activity relative to rest. Sitting quietly is approximately 1 MET. Walking slowly corresponds to roughly 2–3 METs. More demanding activities such as climbing stairs, yard work, or brisk walking fall in the 4–7 MET range. Running or strenuous labor registers at 8 METs and above. The VA uses this scale to translate physical symptoms into an objective, quantifiable measure of functional limitation.
The METs-to-Rating Correlation
The clinical significance of METs documentation lies in its specificity. Symptoms emerging at low METs thresholds indicate severe cardiovascular limitation and correspond to higher disability ratings. Symptoms emerging only at high METs thresholds indicate preserved functional capacity and produce lower ratings. The accuracy of METs data in the medical record therefore depends entirely on whether the documented level reflects the point at which symptoms actually occur—not the maximum physical output a veteran is capable of producing before stopping.
The “Lawn Mower” Trap:
A veteran reports to a physician that yard work is still part of the weekly routine. The physician documents lawn mowing—an activity rated at 5–6 METs—and the record reflects a functional capacity consistent with a 30% or 60% rating. What the record does not capture is that the veteran uses a self-propelled mower and stops every five minutes due to chest pain. The documented activity is accurate; the documented METs tolerance is not. A complete clinical picture requires not only what activities are performed, but the symptomatic limitations that occur during those activities. When this distinction is documented, the clinical records more clearly reflects the veteran’s actual functional limitations.
Left Ventricular Ejection Fraction (LVEF)
While METs measure functional output, LVEF measures the mechanical efficiency of the heart itself. Both metrics are necessary components of a complete cardiac rating picture, and both must be accurately reflected in the clinical record.
The Pump Efficiency Test
LVEF is measured via echocardiogram and expresses the percentage of blood the left ventricle ejects with each contraction. A normal LVEF ranges from 55% to 70%. Under Diagnostic Code 7005, an LVEF below 30% corresponds to a 100% rating regardless of other test results. An LVEF between 30% and 50% falls within the 60% rating tier. Because echocardiographic measurements can vary depending on the equipment and conditions of the exam, records from multiple evaluations—including those obtained through private cardiology practices—provide a more complete picture of cardiac function over time.
Getting Paid While You Recover
The VA’s rating schedule accounts for the period of acute recovery following cardiac surgery. Veterans with service-connected heart conditions are not required to wait until post-surgical stabilization to receive disability compensation.

The Temporary 100% Rule
The VA provides temporary total disability compensation for service-connected conditions requiring surgical treatment and a defined recovery period. This provision reflects the VA’s recognition that the post-operative period represents a state of total disability, irrespective of long-term prognosis.
Immediate Post-Op Status
The placement of a coronary stent—classified as percutaneous coronary intervention (PCI)—qualifies as surgical treatment under this provision. For veterans with established service connection for IHD, a temporary 100% rating applies from the date of the procedure through the designated convalescence period. This is a standard component of the rating process for service-connected surgical interventions.
When the Temporary Rating Ends
The temporary 100% rating typically continues through the end of the third month following the month of hospital discharge. After this period, the VA conducts a re-evaluation to assign a permanent rating based on residual functional measurements—specifically the METs and LVEF data discussed in the preceding sections. A permanent rating at the conclusion of the convalescence period reflects the stable, post-recovery functional baseline.
Building Complete Medical Documentation
The strength of a disability claim is determined not by the severity of the condition alone, but by how completely and accurately that severity is reflected in the documentary record. A diagnosis of IHD, without supporting functional data, does not produce an accurate rating.
Medical Records: Quality Over Quantity
Consolidating both VA and private medical records into a single, comprehensive file ensures the rating authority reviews the complete history of the condition rather than a fragmented subset of it. Gaps in the record—particularly the absence of echocardiographic or stress test data—produce ratings based on incomplete information. The importance of medical evidence in VA disability claims clarifies why the completeness of the clinical record is central to an accurate VA evaluation.
Why Private Records Matter
VA clinical notes are frequently written to reflect care management rather than disability documentation. A notation that a condition is “stable” reflects the absence of acute deterioration—not the presence of preserved functional capacity. Private cardiologist records often contain the granular stress test data and echocardiographic measurements that VA clinical notes omit. When these records are part of the claim file, they provide the specific functional metrics—METs scores, LVEF percentages, symptom frequency—that drive accurate rating determinations.
The “Stable” Misunderstanding:
A VA physician documents a veteran’s cardiac condition as “stable” following a routine visit during which no acute events had occurred. The VA record, reviewed in isolation, suggests a mild, well-managed condition. The veteran’s private cardiologist, however, has documented an inability to walk more than one city block without dizziness—a functional threshold corresponding to approximately 3 METs. When the private cardiology record is included, the full severity of the veteran’s functional limitations is more clearly reflected in the overall record. The VA ultimately assigns a rating based on the totality of evidence in the record.
The DBQ Is Your Blueprint
The Disability Benefits Questionnaire (DBQ) is the structured clinical form that translates a veteran’s medical condition into the standardized format used by VA rating authorities. The DBQ for securing VA benefits explains how this document bridges clinical findings and the rating schedule, and why the specificity of its content is important to accurately reflecting the condition in a standardized format.
Documenting Real-World Limitations
A DBQ that reflects clinical stability rather than a functional limitation may not fully capture the veteran’s day-to-day cardiovascular limitations. The METs level recorded on the DBQ must correspond to the threshold at which symptoms actually occur in the context of daily activities—not the theoretical maximum output achievable in a controlled setting.
Specificity Supports Accuracy
General clinical language produces ambiguous rating determinations. A DBQ that specifies the exact LVEF percentage from the most recent echocardiogram, the precise METs score from stress testing, the frequency and character of angina episodes, and the current medication regimen gives the rating authority the specific data points required for an accurate assessment.
Essential Evidence for the DBQ:
- Exact LVEF percentage from echocardiogram
- Specific METs score from stress test, or clinician-estimated METs based on documented activity tolerance
- Frequency of angina or chest pain episodes
- Complete list of current cardiac medications
- Documentation of cardiac hypertrophy or dilation, if present
The C&P Examination
The Compensation and Pension (C&P) examination is one of the most consequential steps in the rating process and one of the most common points at which functional capacity is inaccurately documented. The VA reviews C&P findings alongside other medical evidence when determining the final rating.

Arriving Prepared
A veteran who can clearly articulate the progression of symptoms, the activities that trigger them, and the limitations those symptoms impose on daily functioning provides the examiner with the clinical narrative necessary to generate accurate documentation. A complete, factual account of symptom history—including the frequency, severity, and duration of cardiac episodes—supports thorough documentation that the VA uses in its evaluation.
Accurate Symptom Reporting
A veteran who suppresses pain signals during a stress test or minimizes symptom reports produces METs data that overstates functional capacity. The examination is a clinical measurement. Accurate reporting of the actual point at which symptoms arise—including chest discomfort, shortness of breath, or dizziness—is the mechanism by which the examiner documents the true functional threshold.
The Parking Lot Observation:
Some veterans, conditioned by military culture to project physical capability, walk briskly from the parking lot to the examination room despite experiencing discomfort. The examiner observes normal gait and no visible shortness of breath upon arrival and documents accordingly. This behavioral pattern inadvertently produces data reflecting higher METs capacity than is clinically accurate. When exertion during transit produces symptoms, communicating that to the examiner upon entering the room ensures the observation is captured in the clinical record.
Clarifying How Activities Are Performed
Examiners sometimes estimate METs capacity based on the types of activities a veteran reports performing, without accounting for the modifications and rest intervals required to complete them. The clinical record is most accurate when documentation reflects not only what activities are undertaken, but the pace at which they are completed, the rest intervals required, and the symptoms that emerge during or after performance.
Understanding VA Review Options
Ischemic Heart Disease is a progressive condition. A rating assigned at one point in time may not accurately reflect severity as the disease advances. When a rating does not correspond to the objective clinical evidence, the VA’s review system provides structured pathways for re-evaluation. How to challenge a low VA rating outlines the available options and the circumstances under which each is most applicable.
| Appeal Lane | Best Used When | Timeline |
| Supplemental Claim | New and relevant evidence exists—such as a stress test documenting lower METs capacity | Avg. 125 days |
| Higher-Level Review | Evidence was already in the record but was not correctly interpreted by the rating authority. No new evidence is introduced. | Avg. 125 days |
| Board Appeal | The dispute involves a complex legal or medical argument requiring review by a Veterans Law Judge | 1 year+ |
Supplemental Claims
According to the VA, veterans may submit a Supplemental Claim when new and relevant evidence—such as a recent echocardiogram reflecting a declining LVEF or a stress test documenting reduced METs tolerance—has not yet been reviewed. This is typically the most direct pathway when updated objective data supports a higher rating tier.
Higher-Level Reviews
Per VA guidance, a Higher-Level Review is available when the existing record contained sufficient evidence to support a different rating, but the initial determination did not accurately reflect that evidence. A senior VA reviewer examines the same record without the introduction of new documentation.
Board Appeals
When a rating dispute involves a nuanced legal argument regarding service connection, secondary connection, or the application of specific statutory provisions, the Board of Veterans’ Appeals provides a formal adjudicative process. This pathway involves longer processing timelines but allows for a more comprehensive review of complex cases.
Rating Increases Over Time
Because IHD is degenerative by nature, functional capacity documented at one point in the disease course may not remain accurate over subsequent years. When clinical indicators reflect meaningful deterioration—including reduced exercise tolerance, increased frequency of angina, or declining LVEF—updated medical documentation reflects current severity and may support VA review of the existing rating.
Don’t Let Bad Data Define Your Rating
Navigating the VA’s rating schedule for a heart stent-related condition is challenging precisely because the outcome depends so heavily on the accuracy of objective functional data. A common source of rating inaccuracy is C&P documentation that overestimates physical capacity due to incomplete clinical questioning or insufficient symptom disclosure during the examination.

REE Medical connects veterans with independent, licensed healthcare professionals who complete Disability Benefits Questionnaires and medical evaluations with a thorough, disability-focused clinical approach. Documentation coordinated through REE Medical is objective and VA-compliant, designed to accurately capture METs tolerance, LVEF data, symptom frequency, and functional limitations in the standardized format the VA uses for rating determinations. For veterans whose cardiac conditions have progressed since their initial rating, independent evaluations through REE Medical’s network generate updated clinical documentation that reflects current functional status.
Veterans can learn more about coordinating independent medical documentation by contacting REE Medical for a complimentary informational consultation about the va disability rating for heart stent evaluation process.
Final Thoughts
A heart stent addresses an acute vascular crisis, but it does not resolve the underlying disease or the functional limitations that disease produces over time. The VA’s compensation framework exists to account for the ongoing impact of that disease on a veteran’s capacity for daily activity—measured objectively through METs and LVEF, and documented through the medical record.
The accuracy of a va disability rating for heart stent evaluation depends entirely on the completeness and specificity of the clinical evidence. When objective test results accurately reflect functional thresholds and the medical record captures the full scope of residual symptoms, the rating authority has the information needed to assign a rating that corresponds to actual disability severity. Veterans who understand how METs and LVEF map to the rating schedule, how to document real-world limitations with clinical precision, and what review options are available when ratings are inaccurate are better positioned to receive compensation that reflects the true impact of their service-connected cardiovascular condition.
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (“VA”). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veteran’s Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.