

VA Rating for Vertigo: Why Claims Are Denied and What the Evidence Record Requires
Vertigo is one of the more frequently misunderstood and underrated conditions in the VA disability system. Claims are often denied or assigned minimum ratings not because the condition is absent, but because the documentation submitted does not align with the specific criteria the VA applies when evaluating vestibular disorders. Veterans commonly describe their symptoms in general terms — dizziness, nausea, loss of balance — without providing the frequency data, functional impact statements, and clinical observations the VA relies on to make accurate rating determinations. This article outlines how the VA evaluates a VA rating for vertigo, where documentation gaps most commonly occur, and how secondary conditions can factor into a veteran’s overall combined rating.
Understanding How the VA Rates Vertigo
The VA evaluates most vertigo claims under Diagnostic Code 6204 (peripheral vestibular disorders), which carries only three rating levels: 10%, 30%, and 100%. At 10%, the criteria require “occasional dizziness.” At 30%, the criteria shift to “dizziness with occasional staggering.” At 100%, the criteria require the veteran to be “bedridden due to dizziness and nausea most of the time.” There is no intermediate rating option between 30% and 100%, which creates a significant gap for veterans with moderate-to-severe chronic vertigo who do not meet the extreme threshold for the highest level.
How the Rating Schedule Applies to Chronic Vertigo
Diagnostic Code 6204 was not designed to account for veterans who experience moderate vertigo episodes multiple times per week. The criteria focus on whether staggering is observable during an examination and whether the veteran is bedridden — neither of which may be apparent during a single Compensation and Pension (C&P) examination on a day when symptoms are temporarily suppressed. The C&P examination provides a snapshot of a single moment in time, and many veterans with episodic vertigo are not experiencing an active episode when examined. When the medical examiner observes no staggering and the veteran is able to ambulate, the rating record reflects that observation regardless of what the veteran’s daily experience involves.
What a Minimum Rating Does Not Reflect
A 10% rating reflects the VA’s acknowledgment that a condition exists — it is not a comprehensive assessment of functional impact. For veterans whose vertigo prevents driving, limits employment options, or produces constant anticipatory concern about the next episode, the 10% threshold may not reflect the full scope of disability. Understanding what evidence is needed for disability claims is foundational to understanding why the medical record — not the veteran’s reported experience alone — determines the rating outcome.
Secondary Conditions Veterans Frequently Overlook
Veterans who receive a 10% vertigo rating often focus their efforts on disputing that rating under the same diagnostic code. A more complete picture of disability may emerge from identifying and documenting secondary conditions that developed as a result of the service-connected vertigo. These conditions are rated separately under their own diagnostic codes and, when properly documented with a clinical opinion connecting them to the primary condition, can significantly affect a veteran’s combined rating.
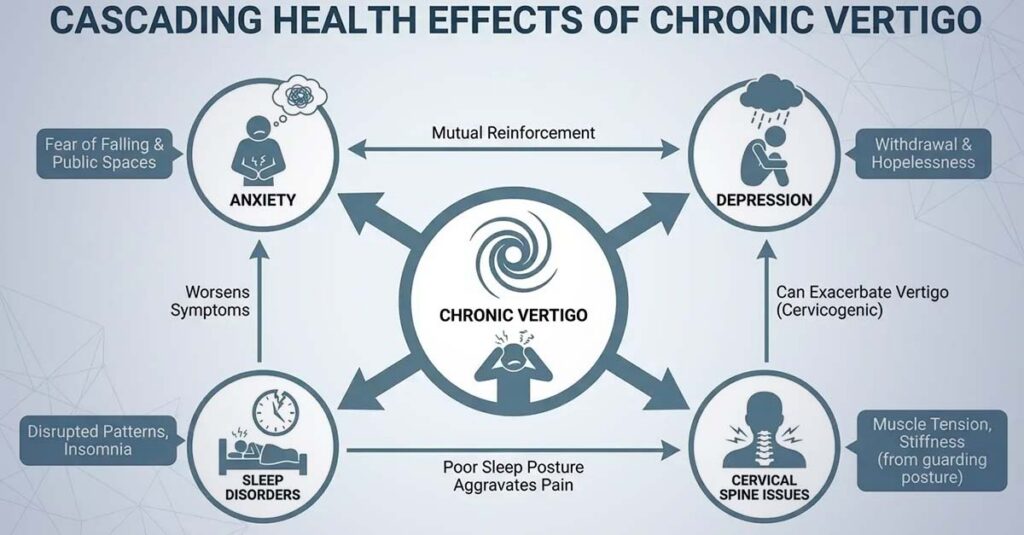
Mental Health Conditions Secondary to Chronic Vertigo
Chronic, unpredictable balance disorders create a specific pattern of psychological impact that mental health professionals recognize as vestibular anxiety. Veterans with this condition become hyperaware of bodily sensations and develop anticipatory concern around activities where a vertigo episode could be dangerous or disruptive. This pattern can progress into panic disorder, agoraphobia, or generalized anxiety disorder — each of which is independently ratable under the VA’s mental health diagnostic criteria.
Depression is another common secondary condition. When vertigo limits a veteran’s ability to drive, work, or participate in social activities, the resulting isolation and loss of independence can produce clinical depressive symptoms. The VA rates anxiety and depression under mental health diagnostic codes that range from 0% to 100% based on functional impairment. Veterans can review information on VA ratings for anxiety to understand how this secondary condition is evaluated and what documentation the VA reviews to assign an accurate rating.
To illustrate how secondary conditions affect a combined rating: a Marine veteran sustained a TBI from an IED blast and was subsequently service-connected for vertigo as a TBI residual, with a 10% rating assigned after a C&P examination that did not document staggering. Three years of mental health treatment records — none of which had been connected to the vertigo claim — documented anxiety and panic attacks that developed in direct response to the unpredictability of his episodes. When a secondary claim for anxiety was filed with those treatment records and a clinical opinion connecting the conditions, the VA ultimately assigned a 50% rating for anxiety. The combined rating increased from 10% to 55%.
Physical Secondary Conditions
The body’s compensatory responses to chronic balance impairment can generate physical secondary conditions that are independently ratable. Veterans who tense the muscles of the neck and shoulders to maintain stability often develop cervical spine strain. Changes in gait associated with balance compensation can contribute to hip, knee, or lower back problems over time. Sleep disorders are another frequently documented secondary condition, as positional vertigo commonly disrupts sleep and many veterans develop insomnia or fragmented sleep patterns as a result.
Common secondary conditions the VA may evaluate in connection with a primary vertigo rating include anxiety disorders, depressive disorders, cervical spine strain, sleep disorders, gastrointestinal conditions related to chronic nausea, and gait-related musculoskeletal problems. Each requires independent medical documentation and a clinical opinion establishing the connection to the primary service-connected condition.
The VA’s Diagnostic Codes for Vertigo
The applicable diagnostic code depends on the underlying cause of the vertigo. Veterans whose vertigo is caused by Meniere’s disease are evaluated under Diagnostic Code 6205 rather than 6204, and the rating criteria differ substantially. Under Code 6205, ratings are assigned based on attack frequency rather than the presence of staggering. The 10% level applies to hearing impairment with attacks of vertigo and tinnitus occurring less than once every few months on average. The 30% level applies to attacks occurring on average once a month. The 60% level applies to attacks occurring on average once a week. The 100% level applies to attacks occurring daily or near-daily.
For veterans with vertigo secondary to a traumatic brain injury, the condition may be evaluated as part of TBI residuals under Diagnostic Code 8045, which uses a functional impairment framework rather than the vestibular-specific criteria of Codes 6204 or 6205. According to VA Claims Insider, VA ratings for vertigo range from 10% to 100% depending on the severity, duration, and frequency of symptoms — making it critical that the correct diagnostic code is applied and that the medical record addresses the specific criteria associated with that code.
What “Occasional” vs. “Constant” Means in VA Terminology
The language used by veterans and their treating providers to describe vertigo symptoms often does not align with the specific definitions the VA applies when evaluating claims. When a veteran reports “constant vertigo,” the VA interprets that phrase as active spinning or dizziness occurring at all times. If an examiner tests the veteran and finds no active vertigo at that moment, the record may reflect “veteran reports constant vertigo but no vertigo observed during exam” — a statement that can affect the credibility of the claim in the VA’s evaluation.
The VA’s frequency definitions are specific. “Occasional” typically means infrequent, generally less than once per month. “Frequent” refers to once per month or more. “Constant” or “near-constant” — the language associated with the highest rating levels under Meniere’s disease criteria — refers to daily or near-daily occurrence.
How Episode Documentation Affects Rating Outcomes
Clinical documentation that specifies episode frequency, duration, and functional impact provides the VA with the data points needed to apply the rating criteria accurately. A medical record that states “patient presents with approximately 8 to 10 vertigo episodes per month, each lasting between 30 minutes and 3 hours, during which the veteran is unable to stand without support and experiences nausea and vomiting” is substantively more useful to the VA’s evaluation than a record that states “patient reports frequent dizziness.”
The following episode-level information reflects the data points the VA reviews when evaluating vertigo claim severity:
- Date and time of episode onset
- Duration in minutes or hours
- Symptoms present during episode (spinning sensation, nausea, vomiting, inability to stand, staggering, tinnitus)
- Activity at time of onset
- Medications taken and their effect
- Time until full resolution
- Impact on activities during and after the episode
The Documentation Gap That Affects Rating Accuracy
Private treating physicians document vertigo from a treatment perspective — they record symptoms, prescribe medications, and monitor the patient’s response. What civilian medical records typically do not reflect is the specific data the VA uses to rate disability: episode frequency quantified numerically, duration data per episode, functional limitation statements written in VA-applicable language, and clinical observations made during an active episode rather than based solely on patient report.
This gap reflects the difference between documentation produced for treatment purposes and documentation produced for disability evaluation purposes. A veteran with extensive treatment records may still have a file that does not contain the evidence the VA needs to assign an accurate rating.
The Role of Objective Vestibular Testing
Objective vestibular testing can provide clinical evidence of dysfunction that supplements the symptom-based record. Videonystagmography (VNG) or electronystagmography (ENG) testing measures eye movement responses to assess inner ear and central motor function. Rotary chair testing evaluates vestibular responses to movement. Vestibular evoked myogenic potential (VEMP) testing can identify structural damage that other tests may not detect. Posturography testing documents balance impairment under varied sensory conditions. Each of these tests generates objective findings that allow the VA to assess vestibular dysfunction independent of self-reported symptoms alone.
The following case illustrates how documentation quality affects outcomes: an Army veteran had been treated for vertigo at a private ENT clinic for two years. Her records contained multiple visit notes, each stating “patient reports ongoing dizziness.” Her initial claim was denied based on absence of objective evidence of severity. Her ENT subsequently produced a detailed letter documenting that over three years of treatment, the veteran had presented with 12 to 15 monthly episodes lasting one to three hours, had not responded adequately to multiple medication trials, and had been examined during active episodes on three occasions with observable nystagmus and inability to perform tandem gait. The VA ultimately assigned a 30% rating on the supplemental claim.
Service Connection: The Prerequisite for Any Rating
A rating cannot be assigned unless service connection is established first. Service connection requires three elements: a current diagnosis, evidence of an in-service event, injury, or exposure, and a clinical opinion connecting the two. All three must be reflected in the evidentiary record.
Pathways to Service Connection for Vertigo
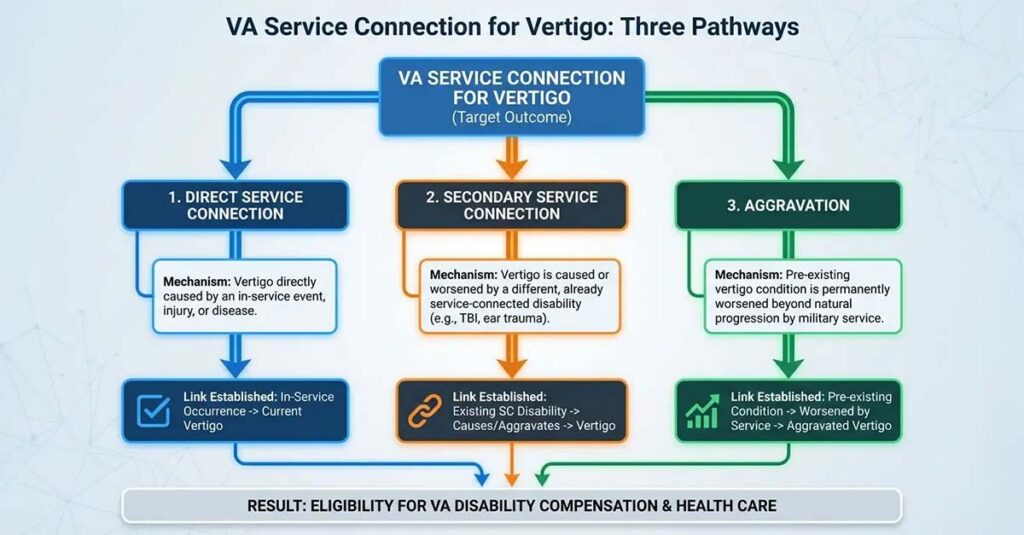
Direct service connection applies when vertigo was caused by an in-service event. Common clinical mechanisms include traumatic brain injury from blast exposure, vehicle accidents, or combat; cervical spine injuries from parachute landings, falls, or physical trauma; acoustic trauma or prolonged noise exposure that damaged inner ear structures; and ototoxic medication exposure during service.
Secondary service connection applies when vertigo was caused or aggravated by a condition that is already service-connected. Vertigo secondary to a service-connected TBI, cervical spine condition, or mental health diagnosis can be established when the clinical record documents both conditions and includes a medical opinion explaining the connection between them.
The Role of Independent Medical Opinions
An independent medical opinion connecting the current vertigo diagnosis to the service-connected event or condition is frequently the pivotal piece of evidence in both approved and denied claims. The opinion must state at minimum that it is “at least as likely as not” — meaning 50% or greater probability — that the veteran’s vertigo is related to the qualifying service event or service-connected condition. It must also provide the medical reasoning behind that conclusion, not merely state it as an assertion.
Treating physicians are often unable or unwilling to produce this type of documentation due to time constraints, liability concerns, or unfamiliarity with VA evidentiary standards. The following elements are typically present in an independent medical opinion that the VA will give weight to in its evaluation:
- Provider’s full name, credentials, and license number
- Provider’s specialty and relevant qualifications
- Statement of what records were reviewed
- Current diagnosis with applicable diagnostic code reference
- Clear statement using “at least as likely as not” language
- Explanation of the medical mechanism linking the service event to the current condition
- Consideration and rebuttal of alternative causes
- Reference to relevant medical literature where applicable
- Provider’s signature and date

How Mental Health Conditions Connect to the Vertigo Record
The clinical connection between chronic vertigo and secondary mental health conditions must be explicitly documented in order for the VA to evaluate and rate the secondary condition. The treatment record should reflect the timeline — documenting that mental health symptoms developed after or concurrent with vertigo onset — and the clinical opinion establishing the connection should explain the mechanism by which the primary condition caused or materially aggravated the secondary condition.
The anxiety that commonly develops in response to unpredictable vertigo involves hypervigilance about bodily sensations, avoidance of situations where an episode could be dangerous, and anticipatory concern about previously routine activities. Over time, this pattern can develop into panic disorder, in which the early sensations of a vertigo episode trigger panic attacks, creating a cycle that worsens both conditions. Depression frequently develops through a separate but related pathway: as vertigo progressively limits driving, employment, and social participation, the resulting isolation and loss of independence produce clinical depressive symptoms that are distinct from — and separately ratable from — the primary vestibular condition.
Filing for a Rating Increase: Evidence Thresholds
A rating increase reflects a material change in condition since the last rating decision — meaning symptoms have worsened in frequency, duration, or functional impact, or new limitations have developed that were not previously documented. Veterans can review the process for requesting a VA disability rating increase to understand the applicable procedures and evidence requirements.
The timing of a filing determines the effective date, which governs how retroactive compensation is calculated. A veteran whose condition significantly worsens in January but who delays filing until June establishes a June effective date. If the claim is approved, back pay is calculated from June — not January. Filing promptly when a material worsening is documented in the medical record preserves the earlier effective date.
The following case illustrates the relevance of timely filing: a veteran with a 10% rating for vertigo secondary to a cervical spine condition experienced a significant escalation in episode frequency in March 2022, progressing from monthly episodes to two or three per week, with visible staggering beginning during episodes. A filing was made immediately in March to preserve the effective date, and the evidentiary record — including updated neurological records, an employer statement documenting work limitations, and video documentation of two episodes showing visible staggering — was submitted in July 2022. The VA assigned a 30% rating in September 2022, with back pay calculated from March.
How REE Medical Coordinates Documentation for Vertigo Claims
A common barrier for veterans with vertigo claims is the absence of a current, thorough independent medical evaluation that documents condition severity and establishes the clinical connection to service in language aligned with VA evaluation standards. VA primary care providers typically do not complete this type of documentation, and private treating physicians may lack familiarity with the specific evidence requirements for VA rating determinations.
REE Medical coordinates access to independent, licensed healthcare professionals who complete DBQs and medical evaluations in accordance with VA formatting and documentation standards. Providers in REE Medical’s network are familiar with disability-focused documentation and VA-standardized forms, with the objective of ensuring that a veteran’s medical evidence accurately and completely reflects the scope of their condition — including episode frequency, functional limitations, and secondary condition connections — before the VA conducts its own review. Veterans can learn more about DBQs for securing VA benefits to understand how structured medical documentation supports accurate rating evaluations.
REE Medical’s flat-rate pricing structure means veterans can access independent medical evaluations without variable or unexpected costs. An informational consultation is available for veterans who want to understand how independent medical documentation is coordinated and what role it plays in the VA’s evaluation process.
Final Considerations
The VA rating for vertigo is governed by specific diagnostic criteria that prioritize observable findings — staggering, episode frequency, and functional incapacitation — over general symptom descriptions. For many veterans, the most productive path toward an accurate combined rating involves not only addressing the primary vertigo claim under the correct diagnostic code, but also identifying and documenting the secondary conditions that chronic vestibular disorders commonly produce.
Documentation is the determining factor. Medical records that specify episode frequency, duration, and functional impact using precise language; diagnostic testing that objectively confirms vestibular dysfunction; independent clinical opinions that explicitly connect the condition to service; and documentation of secondary conditions with clear clinical rationale all contribute to a record that allows the VA to make an accurate determination.
Understanding what evidence is needed for disability claims before engaging with the VA’s evaluation process is one of the most consequential steps a veteran can take toward an accurate rating outcome.
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (“VA”). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veteran’s Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.


