VA Form 21-4192: Understanding the Records Authorization Veterans Often Overlook
VA Form 21-4192 is an authorization form that permits the release of VA medical records to a veteran or a designated party. While the form itself is straightforward, its value in the context of a disability claim is frequently underestimated. Because the VA evaluates claims based on what is documented — not simply what a veteran has experienced — gaps or deficiencies in the medical record can directly affect how conditions are evaluated and rated. This article examines how VA Form 21-4192 works, what it does and does not authorize, and how proactive record review supports a more complete evidentiary record before a claim is submitted.
Why VA Form 21-4192 Exists
The VA maintains internal access to VA medical records, but internal access does not guarantee that those records tell a complete or well-documented story. When a veteran reviews their own records through the process VA Form 21-4192 initiates, the review reveals exactly what is documented — including what is missing, what is vaguely stated, and what may not reflect the actual severity or functional impact of a condition.
The Gap Between Treatment Documentation and Disability Documentation
Treating physicians document care from a clinical perspective: symptoms noted, medications prescribed, follow-up instructions provided. This is not the same as documentation structured to support a VA disability evaluation. The VA rates conditions based on specific data points — frequency, duration, severity scales, functional impact, and range of motion measurements — and standard clinical notes frequently do not capture these details with sufficient specificity.
A veteran who has been treated for back pain for several years may have extensive records that show ongoing treatment but contain no range of motion measurements, no functional limitation statements, and no documentation of how the condition affects work or daily activities. When the VA reviews those records to assign a rating, the record may support only a minimal rating despite the veteran’s actual level of impairment. Reviewing records in advance of filing allows veterans and their representatives to identify these gaps while there is still time to address them. Understanding what evidence is needed for disability claims is foundational to understanding why the quality and specificity of documentation — not its volume — determines how the VA evaluates a condition.
What Happens When VA Form 21-4192 Is Submitted
Submitting VA Form 21-4192 creates an authorization for record release — it does not automatically trigger the delivery of records. The form establishes that the VA facility may release records to the designated party, but a separate follow-up request is typically required to initiate the actual transfer of documents. Veterans who submit the form and then wait passively may find that records are never sent without that follow-up contact.

The Gap Between Treatment Documentation and Disability Documentation
Treating physicians document care from a clinical perspective: symptoms noted, medications prescribed, follow-up instructions provided. This is not the same as documentation structured to support a VA disability evaluation. The VA rates conditions based on specific data points — frequency, duration, severity scales, functional impact, and range of motion measurements — and standard clinical notes frequently do not capture these details with sufficient specificity.
A veteran who has been treated for back pain for several years may have extensive records that show ongoing treatment but contain no range of motion measurements, no functional limitation statements, and no documentation of how the condition affects work or daily activities. When the VA reviews those records to assign a rating, the record may support only a minimal rating despite the veteran’s actual level of impairment. Reviewing records in advance of filing allows veterans and their representatives to identify these gaps while there is still time to address them. Understanding what evidence is needed for disability claims is foundational to understanding why the quality and specificity of documentation — not its volume — determines how the VA evaluates a condition.
What Happens When VA Form 21-4192 Is Submitted
Submitting VA Form 21-4192 creates an authorization for record release — it does not automatically trigger the delivery of records. The form establishes that the VA facility may release records to the designated party, but a separate follow-up request is typically required to initiate the actual transfer of documents. Veterans who submit the form and then wait passively may find that records are never sent without that follow-up contact.
What the Form Covers — and What It Does Not
VA Form 21-4192 authorizes the release of records held by VA medical facilities. It does not authorize the release of service treatment records from the veteran’s time in the military, records from private physicians or hospitals, records from military treatment facilities, or records from other federal agencies. Each of these additional record sources requires a separate request through its own process.
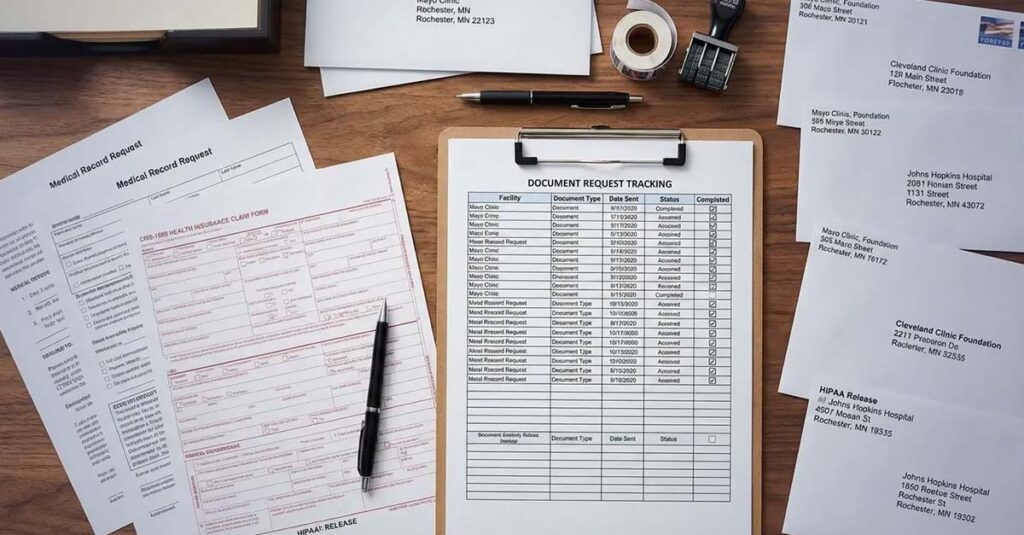
This limited scope is a source of significant confusion. Veterans who believe that a single VA Form 21-4192 submission captures their complete medical history may file claims with an incomplete evidentiary record without realizing it. A thorough record-gathering effort typically involves multiple parallel requests:
- VA medical records — Submitted via VA Form 21-4192 to each VA facility where care was received; records are not automatically consolidated across facilities, meaning separate requests are required for each location
- Service treatment records — Requested through the National Personnel Records Center (for records after 1992) or the relevant service branch archives (for records before 1992) using Standard Form 180
- Private provider records — Requested directly from each private physician, specialist, or hospital using that provider’s own authorization process
- Military treatment facility records — Requested through the specific facility, which may require a separate authorization
- Community care or VA Choice Program records — May be held at the VA facility or may require a direct request to the community provider
A veteran who received care at multiple VA facilities in different states, used private specialists, and has service treatment records spanning several years will need to coordinate multiple independent record requests. Using a VA disability calculator to understand the potential rating impact of each condition can help veterans prioritize which records and conditions merit the most documentation attention.
The Role of Timing in Record Review
The period before a claim is filed is the most effective time to review existing records and address documentation deficiencies. When record review occurs only after a claim is filed — often in response to a VA development letter requesting additional evidence — veterans are working within deadline constraints that compress the time available to obtain new evaluations, identify missing documentation, or address inaccuracies.
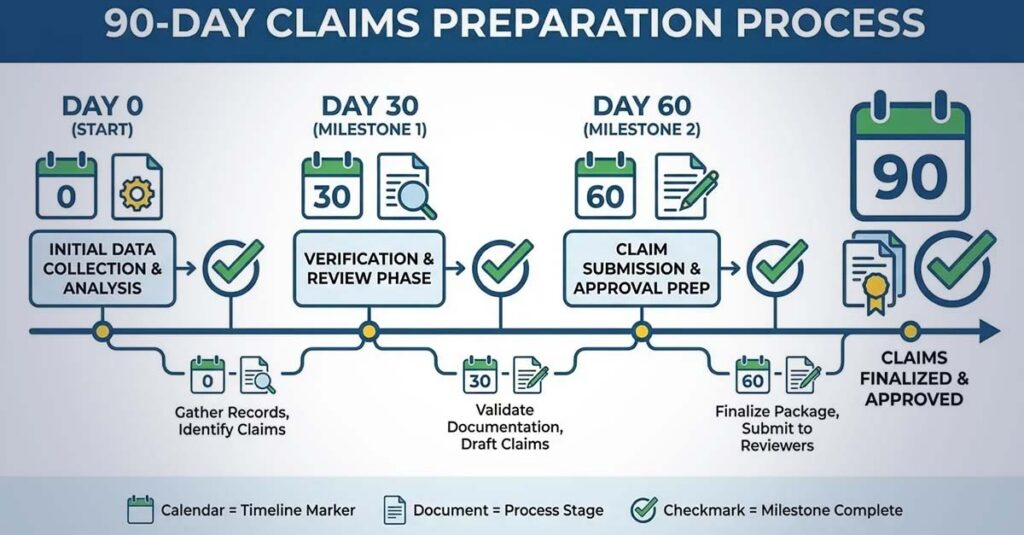
The 60-to-90-Day Framework
Initiating the VA Form 21-4192 request approximately 60 to 90 days before an intended claim filing date accounts for the VA’s processing time, the time needed to receive and review potentially hundreds of pages of records, and the lead time required to address any documentation gaps the review reveals. A veteran who identifies that records lack current range of motion measurements has significantly more options at two months before filing than at two weeks before a VA response deadline.
For veterans who are actively receiving VA treatment, records requested too far in advance may not reflect the current state of a condition. The VA gives more weight to recent evidence for rating purposes, and documentation that is several months old at the time of claim submission may not accurately represent current functional status. The 60-to-90-day window balances preparation time with evidence currency.
To illustrate how this timing affects outcomes: a veteran preparing to file a back claim in September requested records in June and received approximately 180 pages of documentation by July. Upon review, the records showed five years of pain management but no range of motion testing since 2020, no recent imaging, and no documentation of functional limitations. With sufficient time remaining before the planned filing date, updated imaging and a thorough physical examination with range of motion measurements were obtained before the claim was submitted. The claim was filed with both the historical treatment record and current, detailed medical evidence.
Common Misconceptions That Affect Evidence Quality
The VA’s Duty to Assist Has Defined Limits
The VA has a statutory duty to assist veterans in developing claims. This includes requesting records from sources the veteran identifies and, in some cases, ordering a Compensation and Pension examination. However, this duty is narrower than many veterans assume. The VA requests records from sources the veteran lists on the claim — it does not independently investigate to uncover evidence the veteran did not identify. Records that are not requested are not obtained; conditions that are not identified are not evaluated.
Veterans who gather records in advance of filing maintain control over the completeness of their evidentiary record. They are not dependent on the VA’s record requests being fulfilled promptly or completely, and a rating decision is less likely to be made based on a file that is missing significant documentation.
Records Volume Does Not Determine Records Value
A substantial volume of medical records does not necessarily constitute strong evidence for a disability claim. The distinction between high-quality and low-quality documentation lies in specificity. Records that document “patient reports pain” without describing severity, frequency, location, or functional impact give the VA evaluator nothing concrete to work with. Records that document “veteran reports lower back pain at 7/10 severity daily, worsened with standing beyond 30 minutes, with radiation to the left leg; unable to perform lifting requirements of current employment” provide the specific data points the VA needs to apply rating criteria accurately.
When reviewing records obtained through VA Form 21-4192, the relevant questions are: Does the record establish a clear diagnosis? Does it document the condition’s severity with measurable or descriptive specificity? Does it explain how the condition limits function? Does it reflect the condition’s progression over time? Documentation that cannot answer these questions clearly may require supplementation with independent medical evaluations that address them directly.
A Single Request Does Not Capture a Complete History
Veterans who have received care at multiple VA facilities, treated with private specialists, or moved between states will need to submit separate authorization requests to each VA facility and direct requests to each private provider. Records are not automatically consolidated across the VA system. A single VA Form 21-4192 submitted to a veteran’s current VA medical center will not capture records from prior facilities where care was received.
To illustrate the complexity: an Army veteran who separated in 2012 and has since lived in three states may need records from a military treatment facility where surgery was performed during service, the National Personnel Records Center for service treatment records, two prior VA medical centers, a current VA medical center, and a private orthopedic surgeon. That represents six separate record custodians, each with different request procedures and timelines. A single authorization form submitted to the current facility would capture only a portion of the relevant medical history.
Records as Foundation: How VA Form 21-4192 Fits Into a Broader Evidence Framework
VA medical records obtained through this authorization process establish what has been diagnosed and treated over time. They form the historical foundation of a disability claim. However, they are typically not sufficient on their own to support a complete and well-documented claim, particularly for rating purposes.
The VA evaluates a condition’s current severity based on current evidence. Treatment records from prior years may establish the existence and chronicity of a condition, but a rating decision focused on present functional impairment requires current documentation. For veterans whose conditions have worsened since their last VA evaluation, historical records alone will not reflect that change.
Independent medical evaluations and Disability Benefits Questionnaires (DBQs) completed by qualified providers complement the historical record by providing current, structured assessments of condition severity, functional limitations, and — where applicable — the clinical connection between the current condition and military service. These evaluations do not replace VA treatment records; they work alongside them to create a more complete evidentiary picture.

Identifying and Addressing Records Errors
Records review sometimes reveals documentation that is factually inaccurate, inconsistent with a veteran’s actual medical history, or contains language that understates symptom severity. Discovering these issues before filing — rather than after receiving an unfavorable decision — allows time to pursue corrective measures, including requests to amend factually incorrect documentation or to obtain independent evaluations that provide a more accurate and detailed clinical assessment.
The following categories of records issues are worth examining during a pre-claim review:
Accuracy issues: Incorrect diagnoses, wrong dates for injuries or procedures, symptoms attributed to incorrect causes, or procedures documented that were not received
Documentation gaps: Appointments with no corresponding notes, test results referenced in provider notes but absent from the file, imaging ordered without a corresponding radiology report, or specialist referrals with no follow-up records
Quality deficiencies: Vague symptom descriptions without severity or frequency, no functional impact documentation, missing range of motion measurements for joint or spine conditions, no mental health symptom inventories or severity scales, and treatment notes that do not explain why medications were changed or discontinued
Problematic language: Symptoms described as milder than they are, conditions attributed to non-service factors without supporting evidence, or functional abilities overstated relative to the veteran’s actual capacity
How REE Medical Coordinates Independent Medical Documentation
Veterans who review their records and identify documentation gaps — particularly the absence of current severity assessments, functional capacity documentation, or independent medical opinions connecting conditions to service — face the challenge of obtaining supplemental evidence through sources outside the VA treatment system. VA treating providers are focused on clinical care and typically do not produce the type of structured disability documentation that VA rating evaluations require. Private physicians may be willing but unfamiliar with the specific evidentiary standards the VA applies.
REE Medical coordinates access to independent, licensed healthcare professionals who complete DBQs and medical evaluations in accordance with VA formatting and documentation standards. Providers in REE Medical’s network are familiar with disability-focused documentation and VA-standardized forms, with the objective of ensuring that a veteran’s medical evidence accurately reflects the full scope of their condition — including current severity, functional limitations, and where applicable, the clinical relationship between the condition and military service.
This is particularly relevant for veterans pursuing Total Disability Individual Unemployability (TDIU) claims, where the evidentiary record must clearly establish that service-connected conditions prevent substantially gainful employment. When employer records are unavailable or incomplete — according to Hill & Ponton, the VA cannot deny a TDIU claim solely because a former employer did not return a completed employment information form — comprehensive medical documentation that independently establishes work limitations becomes the central evidentiary foundation of the claim.
REE Medical’s flat-rate pricing structure means veterans can access independent medical evaluations without variable or unexpected costs. An informational consultation is available for veterans who want to understand how independent medical documentation is coordinated and what role it plays in the VA’s evaluation process.
Final Considerations
VA Form 21-4192 is not a claim form and does not initiate any rating review. Its value is entirely a function of how the records it produces are used. Veterans who submit the form, receive their records, review them carefully for accuracy and completeness, and then address documentation deficiencies before filing are in a substantially stronger position than those who file without visibility into what the VA’s evaluators will actually see.
The records obtained through this process reveal the gap between what has been clinically documented and what the VA needs to assign an accurate rating. Identifying that gap in advance — rather than discovering it through an unfavorable decision — is the form’s primary value. What happens after that review determines whether the claim is supported by complete, high-quality evidence or submitted with documentation that leaves significant portions of a veteran’s actual functional impairment unaddressed.
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (“VA”). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veteran’s Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.