
VA Rating for Eczema: Understanding How Severity is Evaluated
Eczema is the third most commonly rated skin condition among veterans, with more than 556,000 VA ratings awarded—yet many of those ratings do not accurately reflect the severity of the condition. The VA’s evaluation framework for skin disorders is highly specific, and the gap between what veterans experience daily and what the medical record captures is where underrating most frequently occurs.
This guide breaks down the regulatory and evidentiary landscape that shapes how eczema is evaluated, documented, and rated.
TL;DR
- Diagnostic Code 7806 is the primary rating vehicle for eczema, covering atopic dermatitis, neurodermatitis, and related conditions under a single formula.
- Service connection requires a documented link between the condition and military service—through direct exposure, secondary causation, or aggravation of a pre-existing condition.
- Ratings range from 0% to 60% and hinge primarily on whether treatment involves systemic therapy (oral medications or injections) versus topical creams, and on the percentage of body surface affected.
- Evidence is the determining factor. Because eczema fluctuates, photo logs, medication records, and accurately completed DBQs are critical to establishing severity across the full disease course—not just on the day of examination.
- Pyramiding rules prevent duplicate ratings for overlapping symptoms, but permanent facial scarring from chronic eczema may qualify for a separate rating under a distinct diagnostic code.

The Legal and Medical Reality of Your Skin Claim
Before reviewing rating percentages, it is necessary to understand the legal prerequisites. A diagnosis alone does not produce compensation—the condition must be legally recognized as service-connected, and the clinical record must align with the specific criteria under the applicable diagnostic code. Eczema is the third most commonly rated skin condition among veterans, with more than 556,000 VA ratings awarded, yet many veterans struggle to navigate these legal requirements effectively.
Understanding these foundational elements is what makes a VA rating for eczema evaluation accurate rather than approximate.
Understanding Diagnostic Code 7806
The VA rates dermatitis and eczema under Diagnostic Code 7806, which functions as the primary evaluation framework for atopic dermatitis and related skin conditions. The criteria listed under this code define the specific clinical markers and treatment factors the VA uses to assign a rating percentage. When medical records do not reflect the language and metrics of DC 7806—body surface area percentages, treatment type, and duration—rating accuracy is compromised.
What Symptoms Actually Count
Subjective discomfort alone does not satisfy the evidentiary requirements of DC 7806. The VA looks for objective clinical markers: inflammation, erythema, scaling, vesiculation, and crusting documented consistently across the medical record. Chronicity is equally important—the VA distinguishes between a recurrent, long-term condition and an isolated reactive episode. A single flare without a documented history of recurrence will not support a meaningful rating.
The “Catch-All” Bucket
DC 7806 functions as a broad diagnostic category, covering not only classic atopic eczema but also neurodermatitis, dyshidrotic eczema, and contact dermatitis. Veterans whose diagnosis does not carry the precise label of “eczema” are not necessarily precluded from rating under this code. The unifying factor is the clinical presentation and the applicable rating formula—not the specific sub-classification of the dermatological condition.
Establishing Service Connection
A diagnosis must be linked to military service before any rating can be assigned. Three pathways exist through which eczema may be service-connected.
The Direct Path
Direct service connection applies when medical records from active duty reflect treatment for eczema, and the condition has persisted from that point through the present. A veteran who entered service with clear skin, received treatment for a skin condition during service, and carries that diagnosis today has a documented basis for direct connection.
The Secondary Path
Eczema frequently develops or worsens as a consequence of another service-connected condition. Stress-related flare-ups in veterans rated for anxiety or PTSD are a well-documented clinical pattern. When a service-connected psychiatric or physiological condition demonstrably triggers or exacerbates eczema, a secondary claim supported by an independent medical opinion linking the two conditions reflects that relationship. For veterans already navigating a VA rating for anxiety, identifying how stress exacerbates skin symptoms can be a critical element of establishing secondary service connection.
The Aggravation Path
Veterans who entered service with a pre-existing mild condition may still qualify if military service permanently worsened that condition beyond its natural progression. As noted by Hill & Ponton, the VA may deny service connection if a disability pre-existed service and was not worsened by it—however, if service records do not document the condition upon entry, the Presumption of Soundness places the burden on the VA to demonstrate the veteran was not healthy at the time of enlistment. Proving aggravation requires documentation that the worsening was caused by specific service-related exposures and was permanent—a higher evidentiary standard, but one that objective clinical records can support.
Aggravation in Practice:
A veteran entered the Navy with a history of mild childhood eczema noted on the entrance examination. In the five years prior to service, no medication was required. During a deployment to the Persian Gulf, exposure to JP-8 jet fuel and extreme heat triggered a severe flare-up requiring oral corticosteroids. Post-service, the condition never returned to its mild pre-service baseline and has required continuous treatment since discharge. Documentation of the environmental exposures, the in-service medical treatment, and the permanent worsening of the baseline condition formed the evidentiary foundation for a successful aggravation claim. The VA ultimately assigned service connection based on that documented record.
Cracking the Code on the Rating Schedule
The VA evaluates eczema under the General Rating Formula for Skin Conditions, a framework that disregards subjective pain levels entirely. Ratings are determined by two objective factors: the percentage of body surface area affected by characteristic lesions, and the type and duration of treatment required. Understanding this formula is central to any accurate VA rating for eczema evaluation.
How the General Skin Formula Works
The rating schedule for eczema produces four possible outcomes: 0%, 10%, 30%, or 60%. The transition between these tiers is determined primarily by whether management requires systemic therapy—oral medications or injections—rather than topical applications alone.
VA Eczema Rating Criteria Under Diagnostic Code 7806:
| Rating | Body Area Affected | OR | Treatment Requirement |
| 60% | More than 40% of the entire body or more than 40% of exposed areas | OR | Constant or near-constant systemic therapy over the past 12 months |
| 30% | 20% to 40% of the entire body or 20% to 40% of exposed areas | OR | Systemic therapy for a total duration of 6 weeks or more (but not constant) over the past 12 months |
| 10% | 5% to 20% of the entire body or 5% to 20% of exposed areas | OR | Intermittent systemic therapy for less than 6 weeks over the past 12 months |
| 0% | Less than 5% of the entire body or less than 5% of exposed areas | OR | Requires no more than topical therapy |
Systemic vs. Topical Therapy
The distinction between systemic and topical treatment is the single most consequential variable in the rating formula. Systemic therapy—oral corticosteroids such as prednisone, immunosuppressants, or biologic injections—places a veteran in a higher rating tier regardless of body surface involvement. A veteran managing symptoms exclusively with topical creams, regardless of how extensive or symptomatic the condition, will generally be capped at a lower rating. Pharmacy records documenting the type and duration of systemic medications are therefore essential evidentiary components.

Calculating Body Coverage
When body surface area is the primary rating driver, precise documentation of lesion distribution is required. The VA uses a percentage-of-total-skin calculation. At least 5% coverage is required for a 10% rating; 20% for a 30% rating; and more than 40% for the 60% threshold. This level of specificity requires clinical mapping by a treating physician—a general notation of “extensive involvement” is insufficient for rating purposes.
Frequency and Duration
Duration of systemic therapy within a 12-month period is a defined rating criterion, not an approximation. A 60% rating requires constant or near-constant systemic therapy. A 30% rating requires six weeks or more of systemic therapy within the rating period. Pharmacy records reflecting exact prescription dates, refill history, and medication type provide the objective documentation that supports accurate duration calculations.
The 60% Threshold
The 60% rating is the maximum available under DC 7806 on a schedular basis. It requires either characteristic lesions covering more than 40% of total body surface or exposed areas, or constant and near-constant systemic therapy over the preceding 12 months. This level reflects a condition that is extensive, treatment-resistant, or both.
Defining Incapacitation for Skin Conditions
Unlike orthopedic claims that measure range of motion, skin disability ratings focus on treatment intensity and coverage rather than bed-rest day counts. Hospitalization for eczema lasting more than 21 days may support a temporary 100% rating for that period. Severe flare-ups requiring intensive medical intervention contribute to the clinical picture, but under DC 7806, systemic medication requirements remain the primary rating mechanism.
Facial Disfigurement and Scarring
Chronic eczema that produces permanent disfigurement—particularly on the head, face, or neck—may qualify for a separate rating under DC 7800, which governs scars and disfigurement of the facial area. This rating operates independently of the active eczema rating and is evaluated based on tissue loss and the degree of anatomical distortion. Body scarring under DC 7801–7805 is generally compensable only when the scar is painful, unstable, or covers a substantial surface area. Lichenification—the permanent thickening of skin from chronic scratching—may also meet the threshold for separate evaluation when sufficiently documented.
Building a Complete Evidence Package
Rating criteria are only as useful as the evidence that demonstrates they are met. Because eczema is cyclical by nature, a veteran presenting for examination during a period of remission risks a rating that reflects one day of symptom absence rather than months of documented disease burden. Reviewing what evidence is needed for a disability claim before filing clarifies the full evidentiary framework the VA considers.
The Evidence Foundation
A complete eczema claim requires three categories of documentation: medical context establishing the diagnosis and its clinical history, a professional opinion linking the condition to service, and objective visual evidence of disease severity over time.
Essential Eczema Evidence Checklist:
- Current diagnosis: Medical records confirming atopic dermatitis or eczema
- Independent medical opinion: A clinical statement linking the condition to service, required for secondary claims
- Medication logs: Pharmacy records documenting the duration and type of systemic therapy
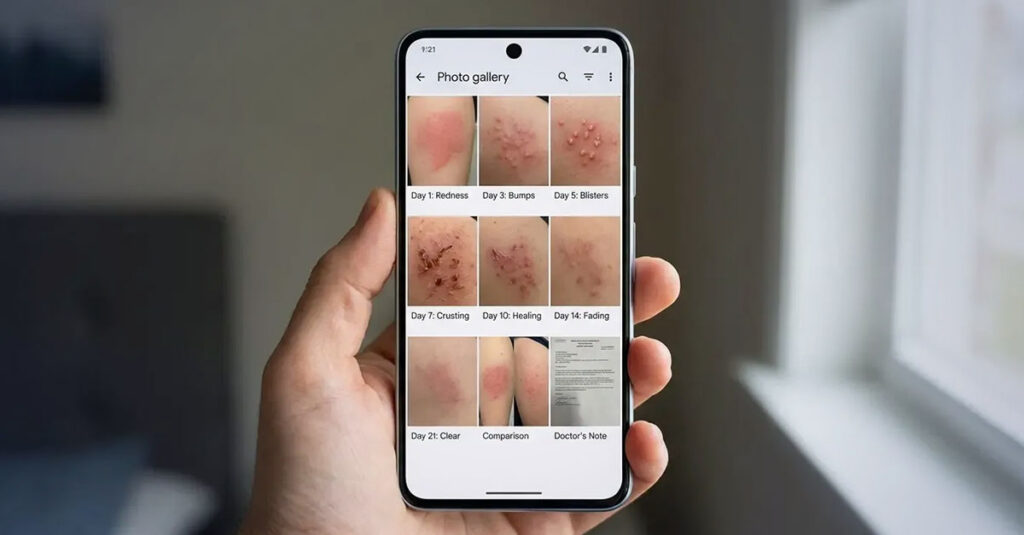
- Color photo log: Dated photographs of flare-ups over a minimum of 3–6 months
- Personal statement (VA Form 21-4138): Detailed account of frequency, sleep disruption, social impact, and functional limitations
- Lay statements: Written accounts from family members or coworkers describing observed symptoms
Personal Statements: VA Form 21-4138
A Statement in Support of Claim submitted via VA Form 21-4138 provides the functional context that clinical records often lack. The statement describes the frequency and severity of flare-ups, the impact on sleep quality due to chronic itching, the social and occupational consequences of visible skin involvement, and any adverse effects of systemic medications. This narrative provides the functional impact context that the VA reviews alongside objective clinical data.
Independent Medical Opinions
For secondary claims—such as eczema attributable to PTSD-related stress or to medications prescribed for a service-connected condition—an independent medical opinion from a licensed physician documents the clinical relationship between conditions. This opinion includes the clinical rationale establishing that the skin condition is at least as likely as not caused or aggravated by the service-connected disability. The language of probability and causal relationship is clinically and legally precise; a general letter of support does not satisfy this standard.
The Photo Log Strategy
Dated, high-resolution photographs of flare-up episodes documented over a 3–6 month period constitute a reliable method of demonstrating disease severity across periods when examination does not coincide with active symptoms. A photo log transforms anecdotal symptom reports into a visual longitudinal record that the VA considers as part of the evidentiary file.
Advanced Strategies for Complex Cases
Some veterans present with disease severity or clinical histories that do not fit neatly within the standard rating tiers. Two mechanisms—temporary total disability ratings and Individual Unemployability—address these circumstances.
The Temporary 100% Rating
Per VA guidelines, hospitalization for a service-connected skin condition lasting more than 21 days entitles the veteran to a temporary 100% rating for the period of hospitalization. In cases where surgical intervention for secondary complications—such as serious skin infections requiring operative management—produces a convalescence period of at least one month during which the veteran cannot work, a temporary 100% rating may also apply. While rare in straightforward eczema cases, severe disease with secondary bacterial or fungal complications can produce these clinical circumstances.

Individual Unemployability (TDIU)
According to the VA, when a service-connected condition does not meet the 100% schedular threshold but nonetheless prevents substantially gainful employment, Individual Unemployability (TDIU) provides compensation at the 100% rate. The evidentiary basis for TDIU requires documentation of how the condition specifically interferes with employment—not a general statement of disability.
| Feature | Schedular Rating | TDIU |
| Criteria | Based on body surface area percentage and medication usage | Based on inability to maintain substantially gainful employment |
| Maximum Rating | 60% under DC 7806 | Paid at the 100% rate |
| Work Status | Compatible with full-time employment | Income generally limited to the federal poverty threshold |
| Best For | Veterans with significant symptoms who remain employed | Veterans whose symptoms prevent hiring or job retention |
Examples of work-related impact may include difficulty wearing required uniforms or PPE, challenges with public-facing work due to visible facial involvement, or difficulty concentrating because of chronic uncontrolled itching.

Pyramiding and the DBQ
The VA prohibits pyramiding—rating the same symptom or clinical manifestation under two separate diagnostic codes. Active eczema lesions and resulting scars in the same anatomical region cannot both be rated if their symptoms are indistinguishable. However, where the active eczema and a permanent scar represent distinct clinical entities—for example, an area of painful, unstable scarring adjacent to but distinct from an active rash site—separate ratings may be appropriate. The VA determines this based on the specific facts and evidence in each case.
The Disability Benefits Questionnaire (DBQ) is the document through which clinical findings are translated into the specific criteria the rating authority applies. Understanding the VA DBQ process explained is essential to ensuring that medical records are rendered in the format the VA requires. A DBQ completed by a physician that explicitly documents systemic therapy duration, body surface coverage percentage, and scarring characteristics provides the rater with the precise data points required for an accurate determination. A general clinical note, by contrast, leaves critical fields unanswered—and absent documentation, the VA evaluates based on what the record reflects.
An incomplete DBQ produces delays and inaccuracies. Every section relevant to the diagnosis must be completed by the examining physician. If the scarring section is left blank, the VA proceeds on the basis that no scarring has been documented.
Accurate Documentation Through REE Medical
Eczema presents a unique evidentiary challenge: the condition is cyclical, and the day of examination may not reflect the severity documented across months of medical records. A C&P examination that coincides with a period of remission produces documentation that reflects one symptom-free day rather than the longitudinal clinical picture.
The “Clear Skin Day” Problem in Practice:
A veteran with chronic eczema experiences severe winter flare-ups requiring oral corticosteroids. Her C&P examination was scheduled in July—her most symptom-free month. The examining physician noted minor dry skin and assigned a 0% rating, without reference to her documented history of winter steroid prescriptions. A DBQ completed by a private physician during a November flare-up documented the full clinical picture—including the history of systemic therapy and the extent of body coverage during active episodes. The VA ultimately assigned a 30% rating based on the totality of evidence in the record.
REE Medical connects veterans with independent, licensed healthcare professionals who complete Disability Benefits Questionnaires and medical evaluations with a thorough, disability-focused clinical approach. Documentation coordinated through REE Medical is objective and VA-compliant, designed to accurately capture systemic therapy history, body surface coverage, symptom frequency, and functional limitations in the standardized format the VA uses for rating determinations. REE Medical operates on a flat-rate, transparent pricing model—no hidden fees and no commissions drawn from future benefit payments.
Final Thoughts
A VA rating for eczema that accurately reflects disease severity requires documentation that captures the condition across its full clinical cycle—not only on the day of examination. The rating formula under DC 7806 is objective and quantifiable, but only when the medical record contains the specific data points the formula requires: systemic therapy duration, body surface coverage, and the chronic nature of the condition.
Documentation Over Time:
A veteran rated at 10% for years had eczema covering 50% of his body surface area but managed it exclusively with topical creams, which limited his rating under the standard formula. A review of his medical history revealed prior prescriptions for oral immunosuppressants that had been discontinued due to adverse side effects. Documentation of the clinical requirement for systemic therapy—even when that therapy was ultimately discontinued—combined with accurate body surface mapping in a new DBQ, provided the VA with updated evidence. The VA ultimately assigned a 60% rating based on the revised evidentiary record.
Veterans whose current compensation does not reflect the actual severity of their condition have formal review options available. How to challenge a low VA rating outlines the pathways through which updated evidence or rating errors may be addressed. Accurate documentation, a complete evidentiary record, and a DBQ that reflects the full clinical picture are the foundational elements of a va rating for eczema evaluation that corresponds to the real-world impact of the condition.
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (“VA”). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veteran’s Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.


