VA Rating for Restless Leg Syndrome: Understanding Analogous Codes and Evidence Requirements
Restless Leg Syndrome (RLS) is one of the most disruptive, yet misunderstood conditions veterans present to the VA. It can impair sleep, focus, energy, and overall quality of life—yet it doesn’t appear anywhere in the VA Schedule for Rating Disabilities. Instead, the VA uses “analogous” diagnostic codes that were designed for other conditions, which often creates confusion about how symptoms translate into disability ratings. This guide examines how the VA approaches RLS, why documentation presents unique challenges, and what evidence matters most when demonstrating the true impact of nightly symptoms. Understanding how the VA evaluates neurological conditions and functional impairment clarifies what documentation is needed to accurately reflect symptom severity.
Executive Summary
RLS does not have its own diagnostic code, so the VA relies on analogous ratings such as Code 8103 (tics) or Code 8620 (neuritis), depending on whether symptoms involve spasms or nerve pain. Because symptoms usually occur at night and are not directly observable during examinations, personal statements and detailed sensory descriptions are essential. RLS can be rated as a primary condition or more commonly as a secondary condition related to medications, iron deficiency, or nerve issues. Bilateral involvement (both legs) may qualify for the VA’s bilateral factor, which increases the combined disability calculation. Independent medical documentation—especially a well-prepared Disability Benefits Questionnaire (DBQ)—can ensure that symptom frequency, severity, and functional impact are clearly recorded for review.

The Challenge of Rating RLS
When veterans lie down exhausted and experience the irresistible urge to move their legs, it destroys sleep and impacts daily functioning. Yet, when examining the VA Schedule for Rating Disabilities (VASRD), no specific entry for Restless Leg Syndrome appears. The schedule hasn’t incorporated this modern sleep medicine diagnosis. This missing entry forces the VA to use a workaround called “analogous rating.” The VA must find the closest match in the existing schedule and apply those criteria. This complicates evaluations because veterans aren’t just proving they have RLS; they must demonstrate their RLS fits criteria designed for a different condition. Understanding what determines your VA rating provides context for how these analogous evaluations work.
The Analogous Rating Process
Since the VA cannot rate unlisted conditions, examiners look for conditions affecting similar body parts or functions. For RLS, the focus is on the neurological system. Codes describing involuntary movements, spasms, or nerve pain become relevant. The rater reviews medical records and determines which existing diagnostic code best captures symptom severity. This decision dictates compensation levels and evidence requirements.
| Rating Feature | Code 8103 (Convulsive Tic) | Code 8620 (Neuritis/Sciatic Nerve) |
| Primary Symptom Focus | Spasms, twitching, and involuntary jerking | Pain, numbness, tingling, and loss of reflexes |
| Best Application | Veterans whose RLS is defined by physical “kicking” or “jerking” of the limbs | Veterans whose RLS is defined by burning sensations or “pins and needles” |
| Rating Basis | Frequency and severity of the tic/spasm | Limitation of motion and sensory deficits |
| Potential Ratings | Typically 0% to 30% (rarely higher) | Can range up to 60% for “severe” cases (though rare for RLS) |
Code 8103: The Convulsive Tic Application
This is the most common pathway for RLS claims. Code 8103 technically covers Tic Douloureux, a condition involving painful facial spasms. However, the VA applies the criteria of this code to legs. Examiners measure the frequency and severity of spasmodic movements. When RLS is defined by the uncontrollable urge to move and physical jerking of limbs, this code is typically applied.
Code 8620: The Nerve Pain Application
Sometimes RLS presents as burning, numbing, or shooting pain rather than twitching. In these instances, the VA might use Code 8620, which covers neuritis of the sciatic nerve. This shifts the evaluation focus. Instead of examining twitch frequency, the rater evaluates how the condition limits motion or causes sensory deficits. It represents a different measurement standard for the same underlying problem.
Documenting an Invisible Condition
When a veteran loses a finger, the VA can see it. If a veteran has a scar, examiners can measure it. RLS is different. It usually occurs when veterans are alone, in the dark, attempting to sleep. A Compensation & Pension (C&P) examiner will likely never observe symptoms during a daytime appointment. This invisibility makes RLS one of the most subjective claims to file. Examiners cannot directly observe the disability; veterans must demonstrate it through descriptions and medical history.
The Personal Statement
Since physicians cannot observe the episodes, veteran descriptions become primary evidence. A Statement in Support of Claim (VA Form 21-4138) details the reality of nightly experiences. Rather than stating “my legs hurt,” the statement explains how sensations force the veteran out of bed at 3 AM and describes the impact on spouses who sleep in separate rooms. This narrative fills the gap that medical testing often leaves.
Information about VA Form 21-4138 clarifies how this document functions for subjective conditions.
VA Form 21-4138 Components:
- Frequency: Exact number of nights per week attacks occur (e.g., “4 to 5 nights weekly”)
- Duration: Time required to fall back asleep (e.g., “Pacing for 90 minutes before sensation subsides”)
- Sensory Details: Descriptive terms like “electric,” “creeping,” or “pulling” rather than generic descriptions
- Social Impact: Information about sleeping in separate beds or fatigue affecting work performance
- Mitigation: Actions taken to alleviate symptoms (e.g., “Hot baths at 2 AM”)

Describing Sensations Accurately
Vague descriptions lead to denials. Specificity about sensations is essential. Veterans often describe pulling, creeping, crawling, or an electric current running through calves. Documenting these specific sensations distinguishes RLS from general leg pain or cramps. It demonstrates to raters that veterans are experiencing neurological events, not simply muscle fatigue.
The Difference Between Weak and Strong Statements:
Weak Statement: “My legs bother me at night and I can’t sleep well. It happens a lot.”
Strong Statement: “Approximately 5 nights weekly, as soon as I lie down, I feel a deep ‘crawling’ sensation inside my calves, like insects moving under the skin. This sensation is not painful but is unbearable, forcing me to stand and pace the hallway for at least an hour until it subsides. My wife now sleeps in the guest room because my thrashing wakes her.”
The Bilateral Factor
RLS rarely affects only one side. It usually attacks both legs. This is significant because the VA has a special calculation for disabilities affecting paired extremities. It’s called the bilateral factor. When veterans receive ratings for left leg and right leg symptoms, the VA doesn’t simply add them to the total. They provide a bonus for the compounded difficulty of having both limbs affected.
The 10% Calculation Boost
The VA combines the ratings for left and right legs to reach a sub-total. Then, they calculate 10% of that sub-total and add it back. Only after this boost do they combine the number with other disabilities (such as tinnitus or PTSD). That additional 10% can sometimes be the precise adjustment needed to move from an 80% overall rating to 90%.
Bilateral Math Application:
A veteran is rated 10% for Left Leg RLS and 10% for Right Leg RLS.
Combined: 10% combined with 10% = 19% (which would normally round to 20%).
Apply Bilateral Factor: The VA calculates 10% of that 19% (which equals 1.9) and adds it to the 19.
New Total: 19 + 1.9 = 20.9.
Result: This 20.9 is then combined with other disabilities. While seemingly small, that extra 1.9 points can be the mathematical factor that rounds the final global rating up to the next highest decile (e.g., pushing an 84% up to an 85%, which rounds to 90%).

Establishing Service Connection
Having a diagnosis isn’t sufficient. Veterans must prove the military caused it. This is the “nexus.” Without this connection, claims cannot proceed. Two primary options exist: proving it started during service, or proving that another service-connected condition is causing it currently.
Direct Service Connection
Direct service connection means claiming the RLS began during active duty. This presents challenges for many veterans because they often didn’t seek medical attention for “restless legs” years ago. They simply endured it. Unless specific medical evidence from time in uniform exists, this pathway is difficult.
Examining Service Records
Veterans can review Service Treatment Records thoroughly. Any documentation related to sleep issues, insomnia, leg cramps, or similar complaints becomes relevant. Even without a diagnosis of RLS, documented complaints of “legs twitching at night” or “inability to sleep due to leg discomfort” can serve as evidence. These notes prove symptoms were present, even when the formal diagnosis was missing.
Continuity of Treatment
When veterans reported leg pain in 2005 but didn’t see a physician again until 2023, the VA may argue the condition resolved and recurred later. Continuity must be demonstrated. “Buddy statements” become valuable here. A letter from a spouse or fellow service member stating they witnessed leg movements consistently over years can bridge gaps in medical records.
Secondary Service Connection
Many veterans find success filing for RLS as a secondary condition. This means the argument isn’t that service caused the RLS directly; the argument is that a service-connected disability (or its treatment) is causing the RLS. This is often easier to prove because medical links are well-established.

Mental Health Medications (SSRIs)
Veterans rated for PTSD, depression, or anxiety can examine their medications. Selective Serotonin Reuptake Inhibitors (SSRIs) and SNRIs are widely known to trigger or aggravate RLS. When these medications are prescribed for service-connected mental health conditions, veterans can link leg symptoms directly to medication side effects.
This is particularly common for veterans who already have a VA rating for depression and what many veterans wish they knew about VA evaluation, as the medications used to treat mood disorders often disrupt dopamine pathways in ways that trigger leg restlessness.
The link between psychiatric medications and RLS is well-documented in medical literature. A case study published in Psychiatry Online detailed a patient who developed severe RLS symptoms within one week of starting clozapine, an antipsychotic. The symptoms were only relieved when an augmenting agent (aripiprazole) was added, highlighting how specific medication adjustments can trigger or resolve the condition. Additionally, Seroquel (quetiapine), commonly prescribed to veterans for depression and bipolar disorder, is known to cause restless leg syndrome as a side effect, alongside other issues like drowsiness and high blood pressure.
Iron Deficiency and Gastrointestinal Issues
The brain requires iron to regulate dopamine, which controls muscle movement. When veterans have service-connected gastrointestinal issues like IBS, GERD, or ulcers, the body might not absorb iron correctly. This leads to low iron levels, which is a primary trigger for RLS. Connecting the gastrointestinal rating to the sleep disorder represents a viable strategy.
Veterans already struggling with IBS or similar gastrointestinal issues may benefit from investigating whether malabsorption is contributing to neurological symptoms.
Back Problems and Nerve Compression
Physical trauma to the spine often leads to neurological issues. When veterans are rated for lumbar strain, herniated discs, or sciatica, nerve compression can manifest as Restless Leg Syndrome. Nerve degradation in the back provides a clear medical pathway to symptoms in the legs.
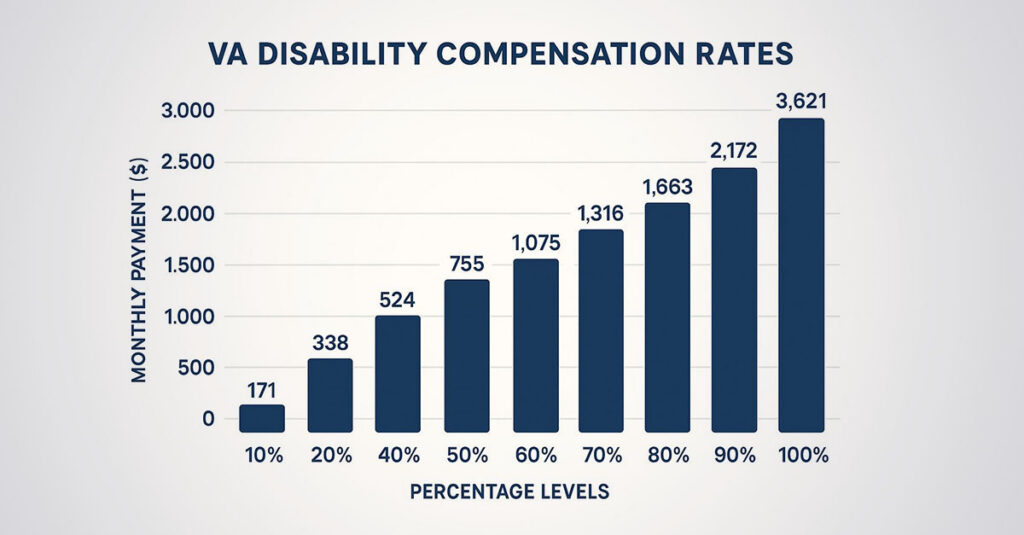
Rating Percentages and Compensation
Once the VA agrees the condition is service-connected, a percentage must be assigned. This number determines monthly compensation. The rating is based entirely on severity—frequency of occurrence and impact on daily functioning.
Rating Breakdown
Under the analogous codes, ratings usually fall into mild, moderate, or severe categories. The VA rater examines evidence to determine placement on the scale.
| Rating Level | Severity Description | Typical Symptoms |
| Mild (10%) | Minimal interference with daily life or sleep | Occasional tingling; managed with basic movement or over-the-counter aids |
| Moderate (20%-30%) | Significant interference with sleep and daily duties | Frequent attacks (several times weekly); requires prescription medication; measurable sleep loss |
| Severe (40%+) | “Marked” interference; loss of reflexes or sensation | Chronic insomnia; muscle atrophy; failure of standard medications; inability to perform work tasks involving sitting |
The 0% to 10% Range
When RLS is manageable, veterans typically receive a 0% or 10% rating. This applies when symptoms are mild, don’t require heavy medication, or don’t significantly impact sleep or work capacity. Service connection is established, but the VA deems the impairment minimal.
The 30% Threshold
To reach higher ratings—typically 30% or sometimes 40% per leg—veterans must demonstrate severe impairment. This means frequent attacks, chronic insomnia, significant distress, and failure to respond to standard treatments. Evidence must show the condition is actively preventing normal functioning.

Critical Evidence Components
Documentation from physicians is required; verbal reports alone are insufficient. The specific document used is the Disability Benefits Questionnaire (DBQ). This form asks specific questions about frequency and severity. When physicians check the “mild” box, veterans receive mild ratings. The accuracy of this document determines outcomes.
The DBQ’s Central Role
The DBQ functions as a scorecard for disabilities. It guides raters on exactly what percentage to assign. When physicians rush through the form or skip sections about how the condition affects daily life, ratings suffer. A detailed, properly completed DBQ differentiates between denials and proper ratings.
Information about the VA DBQ process explained clarifies how this form functions in the evaluation process.
DBQ “Functional Impact” Section:
What the Physician Documents Matters:
Ineffective Note: “Patient reports trouble sleeping.” (Likely 10% rating).
Effective Note: “Patient experiences severe paresthesia nightly, resulting in <4 hours of sleep. Condition prohibits patient from driving long distances or sitting for office work. Prescribed Gabapentin with limited relief.” (Stronger case for 30%+).
Sleep Study Considerations
Sleep studies aren’t strictly required for ratings, but they provide substantial support. A polysomnography can record “Periodic Limb Movements of Sleep” (PLMS). This provides objective data proving legs are moving hundreds of times nightly, even when veterans don’t consciously remember it. It makes claims substantially more difficult to dispute.
Because RLS frequently leads to sleeplessness, a sleep study can also clarify the VA rating for insomnia and understanding the evaluation process, establishing a clear clinical picture of how the movement disorder destroys rest.
Independent Medical Documentation
Most veterans rely on standard C&P examinations arranged by the VA. These appointments typically last 15 minutes with examiners who may not specialize in sleep medicine. When examiners document symptoms as “mild” because veterans didn’t exhibit twitching during daytime examinations, that evidence becomes part of the record. Independent medical evaluations offer an alternative approach.
REE Medical’s Approach to RLS Documentation
REE Medical coordinates access to a network of private physicians familiar with VA regulations. These providers invest time understanding the full scope of conditions. Rather than simply checking boxes, they review medical histories thoroughly.
Comprehensive DBQ Completion
Network physicians complete Disability Benefits Questionnaires (DBQs) with the precision claims require. They ensure RLS severity is documented accurately. When conditions cause severe insomnia and affect work capacity, DBQs reflect that reality. The documentation matches veterans’ actual experiences.
Fully Developed Claims
When veterans submit fully developed claims with comprehensive DBQs from private providers, they provide the VA with necessary evidence from the start. This often eliminates the need for the VA to estimate severity or rely on rushed C&P examinations. Veterans control the narrative before files reach raters’ desks.
Transparent Pricing Structure
REE Medical operates on a flat-rate model with no contingency fees on back pay or future benefits. Veterans know the exact cost for medical evidence generation upfront. Veterans retain 100% of benefits earned through service.
Veterans can learn more about coordinating independent medical documentation by contacting REE Medical for an informational consultation.
Conclusion
Restless Leg Syndrome represents more than a nuisance; it’s a barrier to the rest and recovery veterans need. The VA system is complex, and the lack of a specific code for RLS creates additional navigation challenges. Understanding rating criteria, proper evidence documentation, and the analogous code process supports veterans in pursuing accurate compensation. The VA rating for restless leg syndrome depends on analogous code application, comprehensive symptom documentation, and thorough medical evidence that captures the true impact of nightly neurological symptoms on sleep and daily functioning.
DISCLOSURE
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (“VA”). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veteran’s Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.