VA Rating for Lumbosacral Strain: Understanding the Evaluation Process and Evidence Requirements
Lower back pain represents one of the most common conditions veterans report to the VA, yet it remains one of the most frequently underrated disabilities. The disconnect often stems from how the VA measures impairment rather than whether pain exists. The VA evaluates based on measurable range of motion rather than subjective pain levels. Recent data shows that 21.6 percent of veterans report lower back pain, making this a significant issue across every branch of service. This guide clarifies the VA rating for lumbosacral strain and outlines the evidence requirements that support accurate compensation. Veterans with low ratings can examine how the evaluation criteria work to determine if their rating accurately reflects functional limitations.
Executive Summary
Movement Over Diagnosis: The VA focuses less on diagnostic labels (strain vs. disc disease) and more on Range of Motion (ROM). The Critical Threshold: Forward flexion is the primary driver. Forward flexion of 30 degrees or less is the threshold for 40%. Chain Reaction: Back injuries can legally link to knee, hip, and mental health claims through secondary service connection. Measurement Tools Matter: When examiners don’t use a goniometer (a protractor-like measurement tool), examination accuracy suffers. Worsening Conditions: When back conditions deteriorate, veterans are eligible to file for an increase. Understanding these concepts is the foundation for addressing inadequate lumbosacral strain ratings.

Understanding Back Conditions and Service Connection
Before discussing compensation, the legal groundwork must be established. The VA views back injuries through a specific regulatory lens that differs substantially from how private physicians treat patients. To better understand the process, reviewing the guide on what determines your VA rating explains how the evaluation components fit together.
Clinical Definitions
Veterans often encounter confusion over terminology. Whether classified as a strain, sprain, or disc issue, the rating criteria typically focus on the same factor: functional limitations.
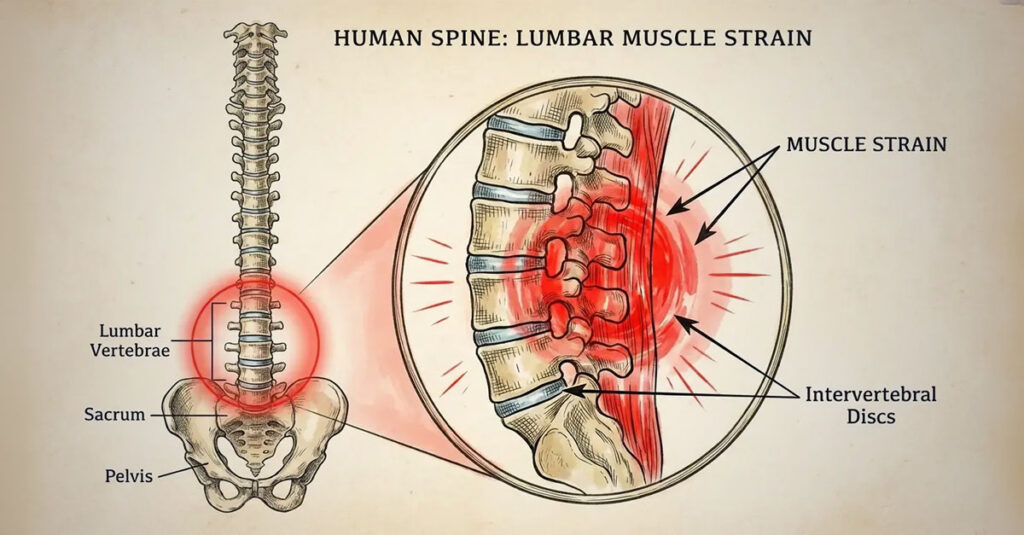
Lumbosacral Strain Defined
Lumbosacral strain is a soft tissue injury to the muscles and tendons in the lower back. It differs from fractures or structural bone damage, but the VA focuses on how that injury restricts movement. Even when physicians diagnose degenerative disc disease, the path to a rating follows largely the same criteria.
Cervical vs. Thoracolumbar: Separate Evaluations
The VA divides the spine into two sections: the neck (cervical) and the lower back (thoracolumbar). These are rated separately. Lumbosacral and cervical strains should be treated as distinct claims. Combining them into one generic “spine” issue may result in missed compensation for one section.
Establishing the Nexus: Linking Pain to Service
A diagnosis holds no weight with the VA without a “Nexus”—the medical connection between military service and current symptoms. Three main pathways exist to prove this connection. Without this medical link, no rating is assigned.

Direct Service Connection: The In-Service Event
This is the most straightforward path. Three elements are required: a current diagnosis, an event during service (such as a fall, jump, or vehicle accident), and a medical opinion linking them. Service treatment records are critical evidence. A 2024 study highlighted that Army personnel report the most back-related injuries, which correlates with rucking and combat support duties.
Aggravation: Service-Worsened Conditions
When veterans entered service with a mild back issue, the concept of “aggravation” applies. The VA compensates for worsening beyond natural progression. The entrance examination is essential documentation to establish the baseline condition.
Secondary Service Connection: The Chain Reaction
When a service-connected back injury causes a new disability (such as knee problems from altered gait), that new disability can also be service-connected. These are termed secondary conditions. This represents a vital strategy for increasing overall compensation.
The Rating Calculation Formula
The VA uses a mathematical formula to determine disability percentages. The primary driver is Range of Motion (ROM). While the calculations are complex, ratings depend almost entirely on these measurements.
The Diagnostic Codes
The VA categorizes injuries using codes. While the code identifies the injury type, it doesn’t necessarily dictate the percentage—symptoms do.
Diagnostic Code 5237 and Related Codes
Code 5237 specifically addresses lumbosacral strain. Related codes include 5242 (arthritis) and 5243 (disc syndrome). Regardless of the code, ratings are generally calculated using the same movement-based criteria.
IVDS and Incapacitating Episodes
Intervertebral Disc Syndrome (IVDS) differs slightly. While typically rated on ROM, IVDS can also be rated based on “incapacitating episodes”—the frequency of periods when the veteran is bedridden. The VA is required to use whichever method produces the higher rating.
Range of Motion: The Measurement Standards
Specific measurements determine ratings. The goniometer (the measuring tool) is essential for accurate assessment.
| Forward Flexion (Degrees) | VA Rating % | Functional Impact |
| > 85 degrees | 0% | Normal movement; no compensation |
| > 60 degrees but ≤ 85 degrees | 10% | Mild limitation; slightly reduced flexibility but functional |
| > 30 degrees but ≤ 60 degrees | 20% | Moderate limitation; distinct stiffness |
| ≤ 30 degrees | 40% | Severe limitation; minimal forward bending ability |
| Frozen Spine | 50% – 100% | Spine is fixed in position (Rare) |
The 10% and 20% Ratings
A 10% rating applies to flexion between 60 and 85 degrees, while 20% applies to flexion between 30 and 60 degrees. When muscle spasms or guarding are present, that can trigger a 20% rating even when motion measurements are slightly better.
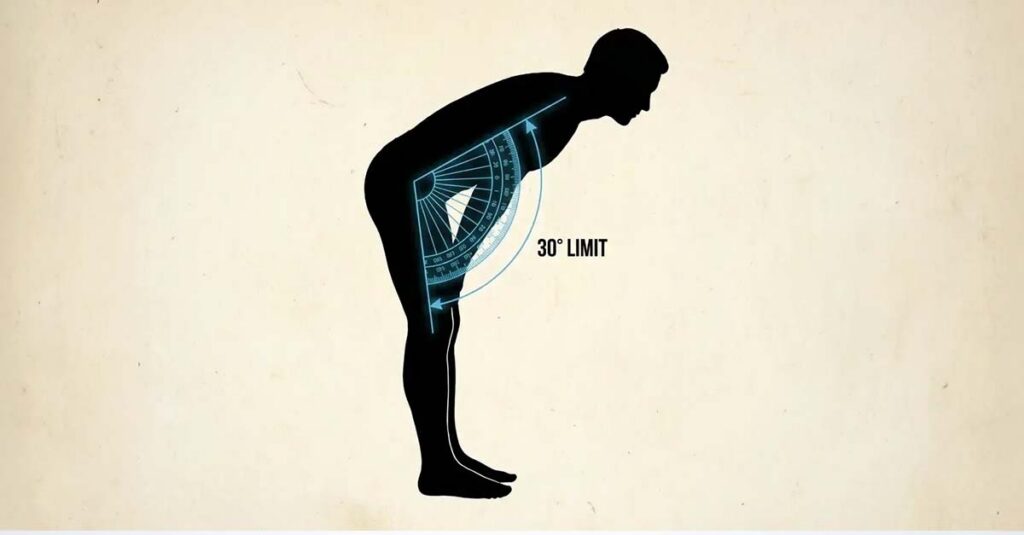
The 30% and 40% Ratings: Severe Restrictions
The 40% rating represents a significant threshold for back claims. The criteria are strict: forward flexion of 30 degrees or less. A 30% rating is a rare middle ground typically involving stiffness in multiple directions.
The Critical Threshold Between 20% and 40%:
Two veterans present for examination. Veteran John bends to 45 degrees during his examination. Because he exceeded the 30-degree threshold, he receives a 20% rating.
Veteran Mike’s measurement stops at 29 degrees. Because his functional limitation kept him under 30 degrees, he receives a 40% rating.
The difference in monthly compensation is substantial, yet physically, their conditions are nearly identical. The 30-degree threshold is the determining factor for the higher rating.
50% and 100%: Unfavorable Ankylosis
“Unfavorable Ankylosis” refers to a spine frozen in a fixed position. A 50% rating applies when the lower back is frozen, while 100% requires the entire spine (cervical and thoracolumbar) to be immobile. These represent rare and severe cases.
The “Flare-Up” Consideration
Back pain isn’t consistent. Ratings shouldn’t reflect only the best functional days. Legal precedents protect veterans who suffer from intermittent severe symptoms.
DeLuca and Mitchell: Pain-Based Functional Loss
Court cases like DeLuca and Mitchell established that examiners must consider functional loss due to pain, weakness, and fatigue. When a rating doesn’t account for how pain limits function during flare-ups, the rating may be inaccurate. Ratings should reflect functional limitations during symptomatic periods.
Repetitive Motion Testing
According to the VA, examiners should request repetitive movements. When range of motion decreases after multiple repetitions due to pain or fatigue, the rating must reflect that reduced range.
Applying the Flare-Up Principle:
Sarah can bend to 70 degrees during asymptomatic periods (corresponding to a 10% rating). However, twice weekly she experiences flare-ups where she can only bend to 25 degrees due to spasms. Under the regulatory framework, the VA examiner should estimate range of motion during flare-ups. When properly documented, Sarah’s rating should reflect her flare-up limitation of 40%, not her 10% baseline.
Secondary Conditions and the Kinetic Chain
A back rating often serves as the anchor for a larger combined claim. The body functions as a kinetic chain—when one component fails, others compensate and eventually fail. Maximizing ratings often involves examining these connections.
Common Secondary Disabilities
Certain conditions are frequently approved as secondary to back strain. Veterans can evaluate their overall health to identify whether other issues stem from service-connected back pain.
| Secondary Condition | Connection to Back Strain | Potential Rating Impact |
| Radiculopathy (Sciatica) | Nerve compression causing radiating leg pain | Rated per leg (10% – 40% each) |
| Knee/Hip Conditions | Altered gait (limping) stresses other joints | Rated per joint based on pain/motion |
| Depression/Anxiety | Chronic pain leads to mental health decline | Typically 30%, 50%, or 70% |
| Erectile Dysfunction | Nerve damage or medication side effects | 0% rating but qualifies for SMC-K (additional monthly compensation) |
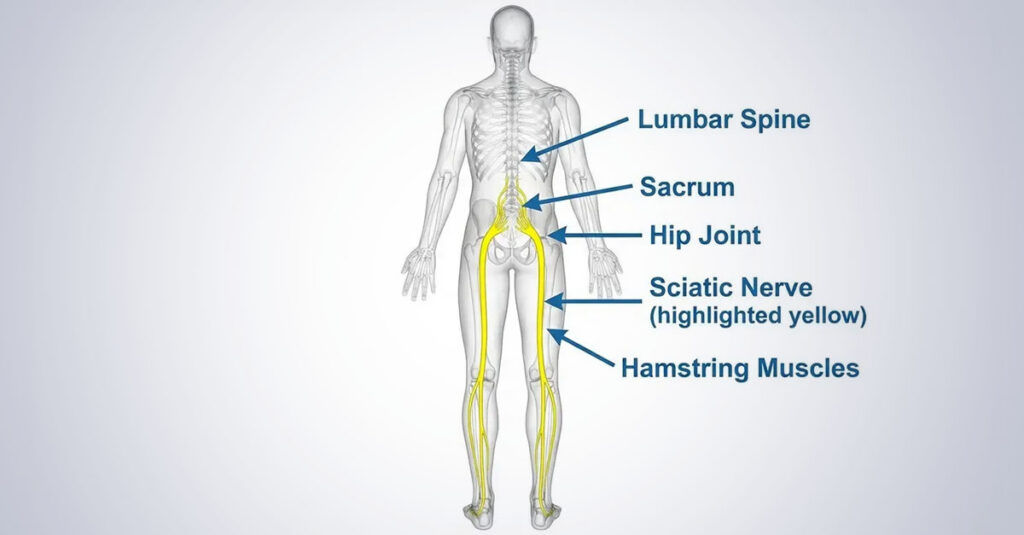
Radiculopathy: Nerve Involvement
Sciatica is common. When back issues compress nerves, causing pain or numbness radiating into the legs, this constitutes a separate condition. Veterans can receive ratings for the back and each affected leg. This can significantly increase overall compensation.
Hip and Knee Issues from Altered Gait
Walking with back pain alters biomechanics. Limping places abnormal stress on hips and knees, leading to orthopedic issues that can be service-connected secondarily.
The Kinetic Chain Effect:
Mark has a service-connected back strain rated at 20%. Because his left side is painful, he shifts weight to his right leg when walking. After five years of this compensatory pattern, his right knee develops arthritis. Mark filed a claim for his right knee secondary to his back. He didn’t need to prove his knee was injured during service; he demonstrated his back injury caused the knee deterioration through altered mechanics.
Mental Health: The Impact of Chronic Pain
Chronic pain frequently leads to depression or anxiety. This can be filed as secondary to the physical injury. The psychological toll is often overlooked but represents a significant component of disability. Veterans experiencing this connection can learn more about the VA rating for depression and what many veterans wish they knew about VA evaluation to determine if this applies to their situation.
Building Evidence for Claims
Documentation determines outcomes. The VA makes decisions based on what exists in the file, not verbal reports alone. Preparation strengthens claims.
Evidence Requirements
Comprehensive Documentation Components:
- Current Diagnosis: Medical records within the last 12 months confirming back strain
- Independent Medical Opinion: Medical assessment linking the diagnosis to service
- Personal Statement: Detailed account of how pain limits daily activities (e.g., cannot tie shoes, cannot stand for extended periods)
- Buddy Letters: Statements from spouse or fellow service members witnessing the injury or daily struggles
- Flare-Up Log: Documentation of the frequency and severity of pain episodes over 30 days
Medical Records: Continuity of Care
Current medical records are essential. Gaps in treatment may suggest the condition has resolved from the VA’s perspective.
DBQs: The Standardized Assessment
The Disability Benefits Questionnaire (DBQ) is the scorecard the VA uses to evaluate conditions. Having a private physician complete a DBQ can provide crucial evidence that may carry more weight than a brief C&P examination. Utilizing a private DBQ for securing VA benefits can document symptoms accurately before the VA makes a determination.
The C&P Examination
The Compensation and Pension examination is the most critical appointment in the evaluation process.

The Goniometer Requirement
When examiners do not use a goniometer to measure range of motion, the examination may lack the precision required for accurate rating. Measurement standards require objective instrumentation.
Filing Strategies
Context enhances raw medical data.
Personal Statements and Buddy Letters
The “Statement in Support of Claim” allows veterans to describe the impact on daily life. Buddy letters verify in-service events and current functional limitations.
The Independent Medical Opinion
An independent medical opinion connects current disability to service. This documentation is often the missing component in denied claims.
Monitoring for Changes Over Time
Back conditions are often degenerative—they typically worsen over time. Data shows that while the number of veterans with low ratings has remained constant, the number of veterans with high ratings is almost seven times higher. This indicates the importance of monitoring worsening symptoms.
Tracking Functional Decline
When range of motion decreases to 30 degrees or less, filing for an increase becomes appropriate. When veterans notice mobility decreasing, information about how to request a rating increase to unlock higher compensation explains the process rather than accepting a rating based on outdated data. Monitoring ratings as conditions progress with age is essential.
REE Medical’s Approach to Back Injury Documentation
Navigating the VA’s evaluation process is complex, and C&P examinations are often rushed or incomplete. REE Medical coordinates access to independent physicians who utilize proper measurement techniques including goniometers and complete DBQs thoroughly. REE Medical specializes in conditions like lumbosacral strain where precise measurements of motion significantly impact financial compensation. REE Medical offers transparent, flat-rate pricing.
Veterans who believe their rating is inaccurate can learn more about coordinating independent medical documentation by contacting REE Medical for an informational consultation.
Conclusion
Compensation for service-connected back pain should reflect functional reality. Back pain affects every aspect of daily life, and VA ratings should accurately represent that impact. Comprehensive evidence and understanding evaluation criteria support accurate ratings. The VA rating for lumbosacral strain depends on documented range of motion measurements, established service connection, and thorough medical evidence that captures functional limitations during both baseline and symptomatic periods.
DISCLOSURE
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (“VA”). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veteran’s Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.