VA Rating for Diabetes: The Truth About Getting the Compensation You Deserve
Veterans navigating the VA rating for diabetes often find themselves overwhelmed by regulations, terminology, and the strict criteria tied to Diagnostic Code 7913. This guide examines how the VA evaluates diabetes—focusing on medical management, lifestyle impact, and documented clinical needs—while highlighting why many veterans receive a lower rating than expected. Whether dealing with Type 1 or Type 2, understanding potential ratings depends on how the condition is treated, what restrictions healthcare providers have identified, and how complications shape the overall disability picture. This article outlines the core principles, rating tiers, and common barriers veterans face when pursuing diabetes-related disability compensation.
Executive Summary
Management over Type: The VA rates diabetes based on how veterans manage it (diet, medication, insulin) and how it restricts daily activities, not strictly on whether they have Type 1 or Type 2. The 40% Threshold: Advancing beyond a 20% rating typically requires insulin dependence and medically documented “regulation of activities.” Secondary Claims Matter: Conditions such as peripheral neuropathy, retinopathy, and renal dysfunction can result in a higher combined rating than the diabetes itself. Presumptive Service Connection: Veterans exposed to Agent Orange (Vietnam, Korea DMZ, Thailand) have a streamlined path to service connection for Type 2 diabetes. Evidence is Critical: Disability Benefits Questionnaires (DBQs) must explicitly document the frequency of doctor visits and specific activity restrictions to support accurate ratings.
Understanding Diagnostic Code 7913
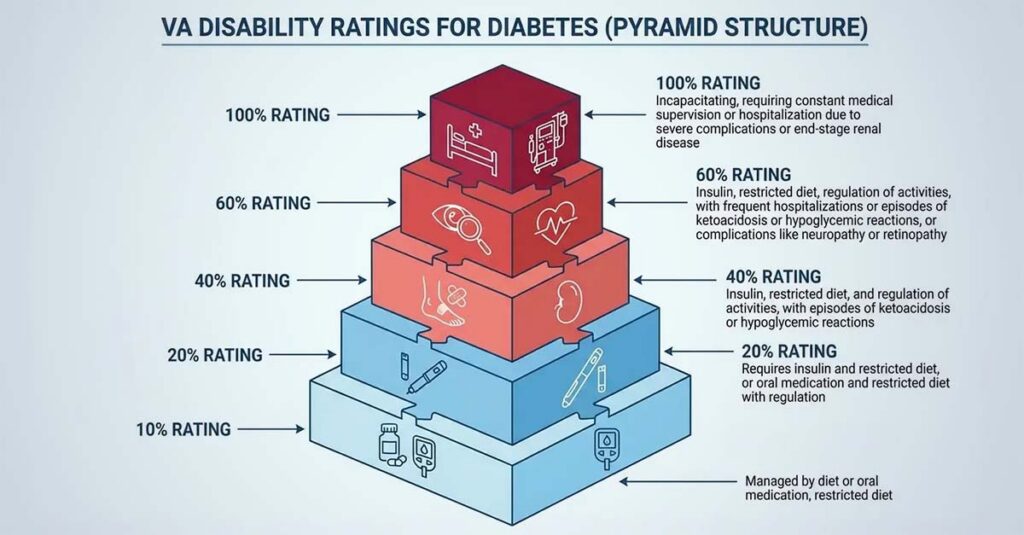
Significant confusion exists regarding how the VA evaluates diabetes. Veterans might assume the severity of their diagnosis determines compensation, but the VA operates under Diagnostic Code 7913, which focuses almost entirely on medical management and lifestyle impact. The VA examines daily management requirements rather than A1C levels alone. The rating scale is rigid—10%, 20%, 40%, 60%, and 100%—and when symptoms fall between categories, the VA typically assigns the lower tier. Understanding the specific requirements for each percentage is essential for accurate compensation.
To better navigate the specific percentages assigned to different conditions, reviewing the basics of understanding VA disability ratings clarifies how the VA calculates overall compensation based on symptom severity.
| Rating | Medical Management Requirement | Key Complications/Restrictions |
| 10% | Restricted diet only | No insulin or oral medications required |
| 20% | Insulin injections OR oral hypoglycemic agent (pills) + restricted diet | No specific activity regulation required |
| 40% | Insulin + restricted diet + regulation of activities | Avoidance of strenuous occupational/recreational activities |
| 60% | Insulin + restricted diet + regulation of activities | Episodes of ketoacidosis/hypoglycemia requiring 1-2 hospitalizations per year OR twice-monthly doctor visits |
| 100% | Insulin + restricted diet + regulation of activities | 3+ hospitalizations per year OR weekly doctor visits; progressive weight/strength loss |
Management Requirements Rather Than Diabetes Type
The regulation doesn’t explicitly differentiate between Type 1 and Type 2, but treatment protocols for each naturally place veterans into different rating categories. The core question raters address is: What does it take to maintain stable blood sugar? Veterans managing their condition through dietary modification receive lower ratings. Veterans requiring insulin and constant medical monitoring to avoid dangerous glycemic episodes receive higher ratings. This represents a functional assessment of dependency on medical intervention.

The 10% and 20% Tier: Diet vs. Medication
Most veterans with Type 2 diabetes receive ratings in these lower tiers. A 10% rating applies when the condition is manageable through dietary restrictions alone—no medications required. Once providers prescribe oral medication or insulin to manage glucose levels, veterans generally advance to the 20% bracket. This represents the baseline for anyone requiring daily medication. While straightforward, this also means that taking Metformin alone doesn’t warrant a high-value rating.
The 40% and 60% Tier: Insulin and Activity Regulation
This is where criteria become strict and where many claims encounter difficulties. To reach 40%, veterans must require insulin, maintain a restricted diet, and have a documented “regulation of activities.” This means healthcare providers have medically advised avoiding strenuous occupational or recreational tasks because they could trigger hypoglycemic events. Claiming reduced exercise isn’t sufficient; medical necessity must be established. For a 60% rating, requirements are even more stringent. Veterans need all previous criteria plus episodes of systemic conditions like ketoacidosis or hypoglycemia that require physician visits twice monthly or more frequently. Without documented proof of these semi-monthly doctor visits, a 60% rating is nearly impossible to secure.
Case Study: The Difference Between 20% and 40%
Veteran A (Rated 20%): Takes daily insulin injections and follows a low-carbohydrate diet. He works an office position and occasionally plays golf. His physician has not placed any formal restrictions on physical exertion.
Veteran B (Rated 40%): Also takes daily insulin and follows a restricted diet. However, he experiences rapid drops in blood sugar during exertion. His physician documented, “Patient must avoid heavy lifting, prolonged walking, and operating heavy machinery due to risk of hypoglycemic syncope.” This medical directive for “regulation of activities” is the determining factor that grants him the higher rating.
The Elusive 100% Rating
100% ratings for diabetes alone are rare because the criteria describe a state of near-constant medical crisis. This level is reserved for “brittle” diabetes. Veterans would need to meet all requirements for 60%, plus demonstrate progressive weight loss and strength reduction, or require hospitalization for ketoacidosis or severe hypoglycemia at least three times annually. Essentially, the condition must remain uncontrolled despite maximum medical therapy.
Type 1 vs. Type 2: Legal vs. Practical Distinctions
Legally, the diagnostic code makes no distinction. Practically, the nature of the disease influences ratings. Veterans sometimes question whether Type 1 automatically receives 100%, and the answer is no. However, because Type 1 is an autoimmune condition that universally requires insulin, these veterans rarely fall below 20%. The distinction matters most when examining claim progression; Type 1 veterans often have an easier time establishing the need for activity regulation, while Type 2 veterans must demonstrate clear deterioration over time.
Type 1 Diabetes and Rating Advantages
Since Type 1 diabetes is insulin-dependent by definition, the baseline rating is typically higher. The argument for “regulation of activities” is often stronger because the risk of rapid, life-threatening hypoglycemia is generally more acute in Type 1 patients than in early-stage Type 2 patients. This makes advancing to 40% more attainable when medical evidence supports restrictions on physical exertion.
The Progressive Nature of Type 2
Type 2 diabetes is the most common form observed in the veteran community. It typically develops gradually. Veterans might be rated at 10% for years while managing it through dietary modification. Eventually, oral medications become necessary, advancing the rating to 20%. Years later, insulin may be required. Documenting these shifts is vital. Veterans cannot remain at a 10% rating if their treatment plan has evolved to insulin dependence. According to the VA, veterans whose medical management has changed may file for an increased rating evaluation.

Establishing Service Connection
Veterans can have severe diabetes, but if the VA doesn’t agree it’s service-related, no compensation is awarded. Establishing this nexus represents the primary hurdle for most veterans. Service connection is evaluated through three pathways: direct evidence from service records, presumptive lists based on deployment locations, or secondary connections linked to other disabilities. Identifying the applicable pathway before filing is essential.
Because the burden of proof rests with veterans to demonstrate the origin of the condition, understanding the importance of medical evidence in VA disability claims is critical for establishing a solid nexus.
Evidence the VA May Review for Service Connection:
- Service Treatment Records (STRs): Glucose readings, urinalysis results showing elevated sugar, or early diagnosis
- DD-214: Verification of service locations for presumptive eligibility (Vietnam, Korea DMZ, etc.)
- Independent Medical Opinion: Medical assessment linking current diabetes to service or a service-connected condition
- Buddy Statements: Letters from fellow service members describing symptoms during service (excessive thirst, fatigue)
- Private Medical Records: Complete history of diagnosis and progression since discharge
The Agent Orange Connection (Presumptive)
Veterans who served in Vietnam, the Korean DMZ, or certain bases in Thailand during specific timeframes benefit from presumptive service connection. The VA presumes Type 2 diabetes was caused by herbicide exposure (Agent Orange). This streamlines service connection. Veterans don’t need to prove a specific event caused the disease; they simply need to prove boots-on-ground presence in the eligible location and possess a current diagnosis. This also applies to Blue Water Navy veterans who served offshore.
Connecting Diabetes to Other Disabilities (Secondary)
This represents a critical strategy for veterans who developed diabetes years after discharge and don’t meet Agent Orange criteria. When a service-connected condition caused diabetes, veterans can file a secondary claim. This pathway is frequently successful. It requires a medical opinion linking the two conditions, but it opens access to compensation that would otherwise be denied.
Example: The Obesity “Intermediate Step”
Sarah, a mechanic in the Army, suffered a severe back injury (service-connected at 40%). Because of chronic pain, she became sedentary and gained significant weight (obesity). This obesity eventually led to Type 2 Diabetes development. While obesity itself is not a rated disability, Sarah successfully claimed diabetes as secondary to her back injury. Her argument: The service-connected back pain caused the obesity, which in turn caused the diabetes.
The Mental Health and Obesity Link
Medications for PTSD, depression, or anxiety often have metabolic side effects leading to significant weight gain. Obesity itself isn’t a rated disability, but it can be an “intermediate step.” When service-connected PTSD medication caused obesity, and that obesity caused Type 2 diabetes, a valid claim path exists.
Aggravation of Pre-Existing Conditions
Veterans who had pre-diabetes before enlisting may still qualify if service worsened the condition. More commonly, “aggravation” occurs where a service-connected orthopedic injury (such as damaged knees or back injury) prevents exercise. This sedentary lifestyle, forced by a service injury, can aggravate or accelerate diabetes development.

The Direct Route: In-Service Evidence
Veterans without presumptive status or a secondary link must pursue the direct route. This requires examining Service Treatment Records (STRs) for elevated blood sugar readings, glucose in urine during physicals, or formal diagnosis while on active duty. Without this documentation trail, a direct service connection is extremely difficult to establish.
Secondary Conditions and Combined Ratings
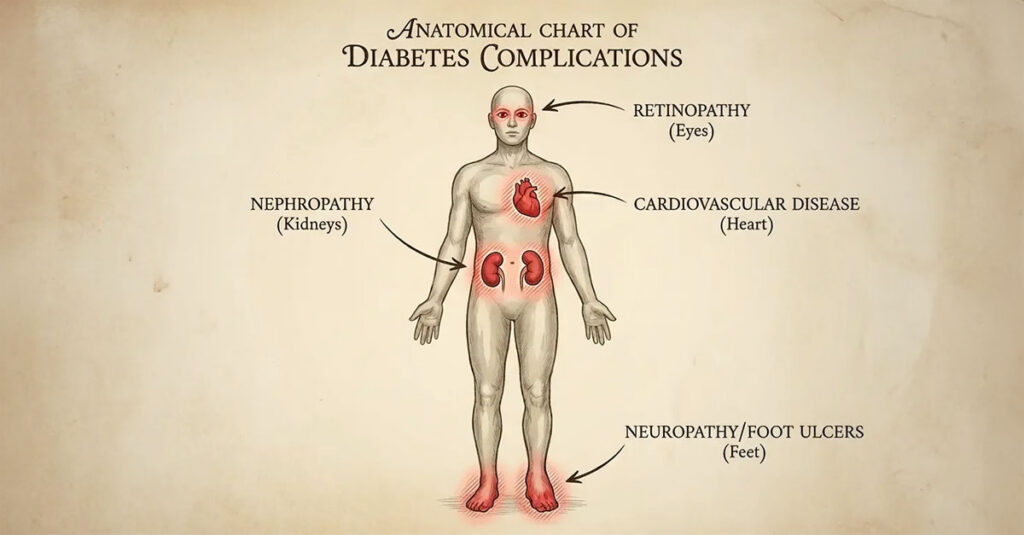
Strategic claim management becomes nuanced when addressing secondary conditions. Diabetes is a systemic disease—it damages nerves, blood vessels, and organs. Ratings for these complications (secondary conditions) often exceed the rating for diabetes itself. Veterans rated for diabetes should be evaluated for related complications affecting other body systems.
| Secondary Condition | Connection to Diabetes | Potential Rating Impact |
| Peripheral Neuropathy | Nerve damage due to chronic hyperglycemia | Rated per limb (hands/feet); can result in 4 separate ratings |
| Diabetic Retinopathy | Damage to retinal blood vessels | Rated based on visual impairment/blindness |
| Renal Dysfunction | Nephropathy affecting kidney function | Can reach 100% if dialysis is required |
| Erectile Dysfunction | Impaired blood flow and nerve function | 0% rating typically, but qualifies for SMC-K (additional monthly compensation) |
| Heart Disease | Increased cardiovascular risk | Rated based on METs testing and cardiac function |
Diabetic Peripheral Neuropathy
Chronic hyperglycemia destroys nerves, typically beginning in the extremities. This is called peripheral neuropathy. The VA rates each limb separately. Veterans experiencing numbness, tingling, or pain in both hands and both feet can receive four separate ratings that combine mathematically. Severe neuropathy can easily exceed the rating of the diabetes that caused it.
Vision, Kidneys, and Cardiovascular Issues
The damage extends beyond nerves. Diabetic retinopathy can lead to blindness and is ratable based on visual impairment severity. Diabetic nephropathy (kidney dysfunction) is rated on renal failure severity, potentially reaching 100% if dialysis becomes necessary. Furthermore, the link between diabetes and cardiovascular disease is well-established. Veterans with service-connected diabetes who develop heart disease or hypertension should claim those conditions as secondary.
Because cardiovascular issues are a common complication, reviewing resources on heart health for heroes and tips every veteran should know can assist in identifying symptoms that may warrant a secondary claim.

The Role of DBQs and C&P Examinations
Veterans cannot simply report illness; they must provide evidence on VA-standardized forms. The Disability Benefits Questionnaire (DBQ) is the instrument the VA uses to capture condition severity. The quality of data on this form directly correlates to rating accuracy. Vague documentation results in lower ratings.
To ensure full preparation for how these forms impact claims, reviewing the guide on the VA DBQ process explained clarifies exactly what examiners evaluate.
The DBQ as Documentation Foundation
The DBQ asks specific questions that map directly to the rating criteria discussed earlier. It addresses insulin usage, frequency of doctor visits, and activity restrictions. While VA physicians complete these during Compensation and Pension (C&P) examinations, veterans have the right to submit DBQs completed by private physicians.
DBQ Documentation Requirements for Higher Ratings:
- Insulin Confirmation: Form clearly states “Requires insulin”
- Frequency of Visits: Visits for “diabetic care” documented as occurring 2x/month or weekly (for 60% or 100%)
- Hypoglycemic Episodes: Specific dates of hospitalizations or ER visits listed
- Activity Restrictions: Physician explicitly documents why strenuous activities cannot be performed (e.g., “Risk of syncope,” “Unable to regulate glucose during exertion”)
- Secondary Conditions: Complications like neuropathy checked and evaluated

Private Physicians vs. VA Examiners
VA-contracted examiners may conduct appointments lasting 15 minutes. They lack familiarity with complete medical histories and often face scheduling pressures. Private physicians can invest time reviewing entire medical files. They can ensure details like “regulation of activities” are not merely checked off, but explained with medical reasoning. This independent medical evidence often determines the difference between denial and approval.
The C&P Examination
The C&P exam is not a treatment appointment; it is a forensic evaluation. Downplaying symptoms can be detrimental. This is not the time for stoicism. When veterans tell examiners “I’m doing okay,” examiners document that the condition is well-managed and asymptomatic. Honest reporting about worst-case scenarios, not best-case scenarios, is essential.
Defining “Regulation of Activities”
To reach the 40% threshold, veterans must articulate functional limitations. Vague statements are insufficient. Specific explanations are necessary: “I cannot go on long hikes, I cannot lift heavy weights at work, and I cannot perform strenuous yard work because my blood sugar drops dangerously low.” When examiners don’t document that activities are medically restricted, ratings typically remain at 20%.
Example: Articulating Restrictions
During his C&P exam, Robert was asked if he exercises. Instead of responding “No,” he explained: “I used to hike every weekend. Now, my doctor has strictly forbidden me from hikes longer than 30 minutes because my blood sugar crashes rapidly, and I’ve passed out on the trail twice. I am medically restricted from any cardio that raises my heart rate for extended periods.” This specific detail supports the “regulation of activities” requirement for a 40% rating.

Obtaining Accurate Disability Ratings
Diabetes impacts the ability to work, vision, nerve function, and daily freedom. Yet veterans are consistently underrated because standard VA examinations overlook regulatory nuances. They miss secondary conditions or fail to document the necessity of activity regulation. Veterans deserve ratings that accurately reflect the true severity of their conditions.
Veterans who believe their compensation doesn’t reflect their condition’s severity can learn more about how to challenge a low VA rating as a potential step toward rectifying the decision.
REE Medical’s Approach to Diabetes Documentation
Veterans deserve ratings that reflect the true severity of their conditions. REE Medical coordinates access to a network of independent, licensed medical professionals who specialize in completing accurate, comprehensive Disability Benefits Questionnaires (DBQs).
These providers invest time understanding management regimens, ensuring the distinction between a 20% and 40% rating is clearly documented. REE Medical also coordinates evaluation of secondary complications like neuropathy, which can significantly increase overall compensation. By submitting thorough, VA-compliant DBQs from neutral third parties, veterans provide their claims with the objective evidence needed for accurate evaluation.
Veterans who believe their current rating is inaccurate, or who are filing for an increase, can learn more about coordinating independent medical documentation by contacting REE Medical for an informational consultation.
Conclusion
Navigating the VA rating for diabetes is complex, but it follows established patterns. Understanding Diagnostic Code 7913 and ensuring medical records reflect required management is essential. Whether establishing the need for insulin and activity regulation or linking secondary conditions like neuropathy, the burden of proof rests with veterans. The VA rating for diabetes depends on documented evidence, not assumption. Comprehensive medical documentation, understanding regulatory criteria, and obtaining thorough independent medical evaluations all contribute to securing ratings that accurately reflect service-connected conditions.
DISCLOSURE
DISCLAIMER: REE Medical, LLC is not a Veterans Service Organization (VSO) or a law firm and is not affiliated with the U.S. Veterans Administration (“VA”). Results are not guaranteed, and REE Medical, LLC makes no promises. REE Medical’s staff does not provide medical advice or legal advice, and REE Medical is not a law firm. Any information discussed, such as, but not limited to, the likely chance of an increase or service connection, estimated benefit amounts, and potential new ratings, is solely based on past client generalizations and not specific to any one patient. The doctor has the right to reject and/or refuse to complete a Veteran’s Disability Benefit Questionnaire if they feel the Veteran is not being truthful. The Veteran’s Administration is the only agency that can make a determination regarding whether or not a Veteran will receive an increase in their service-connected disabilities or make a decision on whether or not a disability will be considered service-connected. This business is not sponsored by, or affiliated with, the United States Department of Veterans Affairs, any State Department of Military and Veterans Affairs, or any other federally chartered veterans service organization.